Download
1 / 1
10 likes | 159 Views
Sensor and Sampling-based Motion Planning for Minimally Invasive Robotic Exploration of Osteolytic Lesions. Johns Hopkins University. Applied Physics Lab. Wen P . Liu a , Blake C. Lucas a,b , Kelleher Guerin a , Erion Plaku c a Department of Computer Science, Johns Hopkins University

E N D
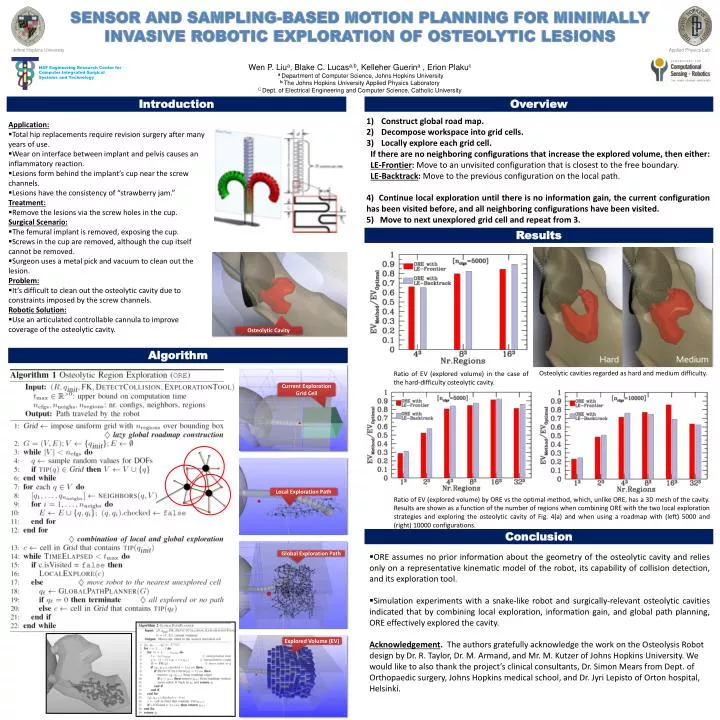
Sensor and Sampling-based Motion Planning for Minimally Invasive Robotic Exploration of Osteolytic Lesions Johns Hopkins University Applied Physics Lab WenP. Liua, Blake C. Lucasa,b, Kelleher Guerina, ErionPlakuc aDepartment of Computer Science, Johns Hopkins University bThe Johns Hopkins University Applied Physics Laboratory C Dept. of Electrical Engineering and Computer Science, Catholic University NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology Introduction Overview • Construct global road map. • Decompose workspace into grid cells. • Locally explore each grid cell. • If there are no neighboring configurations that increase the explored volume, then either: • LE-Frontier: Move to an unvisited configuration that is closest to the free boundary. • LE-Backtrack: Move to the previous configuration on thelocal path. • 4) Continue local exploration until there is no information gain, the current configuration has been visited before, and all neighboring configurations have been visited. • 5) Move to next unexplored grid cell and repeat from 3. • Application: • Total hip replacements require revision surgeryafter many years of use. • Wear on interface between implant and pelvis causes an inflammatory reaction. • Lesions form behind the implant’s cup near the screw channels. • Lesions have the consistency of “strawberry jam.” • Treatment: • Remove the lesions via the screw holes in the cup. • Surgical Scenario: • The femural implant is removed, exposing the cup. • Screws in the cup are removed, although the cup itself cannot be removed. • Surgeon uses a metal pick and vacuum to clean out the lesion. • Problem: • It’s difficult to clean out the osteolytic cavity due to constraints imposed by the screw channels. • Robotic Solution: • Use an articulated controllable cannula to improve coverage of the osteolytic cavity. Results Osteolytic Cavity Algorithm Osteolytic cavities regarded as hard and medium difficulty. Ratio of EV (explored volume) in the case of the hard-difficulty osteolyticcavity. Current Exploration Grid Cell Local Exploration Path Ratio of EV (explored volume) by ORE vs the optimal method, which, unlike ORE, has a 3D mesh of the cavity. Results are shown as a function of the number of regions when combining ORE with the two local exploration strategies and exploring the osteolytic cavity of Fig. 4(a) and when using a roadmap with (left) 5000 and (right) 10000 configurations. Conclusion Global Exploration Path • ORE assumes no prior information about the geometry of the osteolytic cavity and relies only on a representative kinematic model of the robot, its capability of collision detection, and its exploration tool. • Simulation experiments with a snake-like robot and surgically-relevant osteolytic cavities indicated that by combining local exploration, information gain, and global path planning, ORE effectively explored the cavity. • Acknowledgement. The authors gratefully acknowledge the work on the Osteolysis Robot design by Dr. R. Taylor, Dr. M. Armand, and Mr. M. Kutzer of Johns Hopkins University. We would like to also thank the project’s clinical consultants, Dr. Simon Mears from Dept. of Orthopaedic surgery, Johns Hopkins medical school, and Dr. JyriLepisto of Orton hospital, Helsinki. Explored Volume (EV)