Download
1 / 15
170 likes | 662 Views
VATS Mediastinal Lymph Node Dissection AATS Focus on Lung Cancer Boston Nov 2012. Scott J. Swanson, M.D. Director Minimally Invasive Thoracic Surgery Brigham and Women’s Hospital Professor of Surgery Harvard Medical School. Disclosures. I have no conflicts for this talk

E N D
VATS MediastinalLymph Node DissectionAATS Focus on Lung CancerBoston Nov 2012 Scott J. Swanson, M.D. Director Minimally Invasive Thoracic Surgery Brigham and Women’s Hospital Professor of Surgery Harvard Medical School
Disclosures • I have no conflicts for this talk • I serve as a consultant to Covidien and Ethicon
Most Important Principles of Surgical Management of Non-Small Cell Lung Cancer • Clear Surgical Margin • Sampling/Dissection of Lymph Nodes
Lymph Node Sampling versus Dissection is Controversial Wolf AS, Richards WG, Jaklitsch MT, Gill R, Chirieac LR, Colson YL, Mohiuddin K, Mentzer SJ, Bueno R, Sugarbaker DJ and Swanson SJ. Lobectomy versus sublobar resection for small (2 cm or less) non-small cell lung cancers. Ann Thorac Surg. 2011 Nov;92:1819-23. Presentation of Z0030 trial at AATS 2010 suggested no added benefit to dissection after careful sampling in early stage lung cancer However careful sampling is of critical importance for staging and possible improvement in outcome Data suggests inadequate sampling is associated with worse outcome Ludwig MS et al. Postoperative survival and the number of lymph nodes sampled during resection of node-negative NSLC. Chest 2005. 1545-50.
Methods for Assessment CXR Chest CT scan CT/PET EBUS/EUS Mediastinoscopy VAMLA Open lymphadenectomy Sentinel node sampling
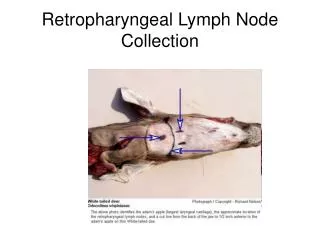
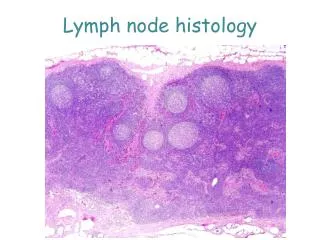
Technique of Mediastinal Lymph Node Dissection Right Paratracheal – clear all tissue from SVC to trachea and from upper lobe bronchus to the subclavian artery Left Aorto-Pulmonary Window –clear all tissue from phrenic nerve to the descending aorta and from the left upper lobe bronchus to the subclavian artery Subcarinal- clear out all tissue bordered by the right and left bronchi and pericardium
Mediastinal Node Dissection Shapiro M, Weiser TS, Wisnivesky JP, Chin, Arustamyan M and Swanson SJ. JTCS 2009 Whitson BA, Groth SS, Duval S, Swanson SJ and Maddaus M. Ann Thorac Surg 2008 Yan TD, Black D, Bannon PG, McCaughan BC. J. Clin Onc 2009 Either VATS or thoracotomy for exposure Data for local recurrence and survival shows no difference between these techniques 2 meta- analyses raise possibility of VATS superiority
Standard Approach CT/PET Various algorithms but most have mediastinoscopy Question true utility of mediastinoscopy/mediastinal staging for early peripheral lung cancer with negative CT/PET scan of mediastinum There may be a VATS alternative which is oncologically sound and saves operative time and morbidity related to mediastinoscopy
One approach • For outer half lung cancer with negative CT/PET scan in the mediastinum • Begin VATS lobectomy with ipsilateral mediastinal node evaluation (N2) • For right sided tumors – 2R, 4R, 7, 8, 9 • For left sided tumors – 5,6, 7, 8, 9 • Evaluate by rapid section, if (+) stop and go to induction therapy prior to lobectomy • In my experience this is less than 5% • Potential downside is skip to N3 with negative N2 which would have been picked up on mediastinoscopy – I have not seen this i.e. in following pts none have recurred in contralateral mediastinum or false negative frozen section result
Conclusions VATS lymphadenectomy is easy to accomplish and effective Lymph node assessment and treatment is of the utmost importance in moving the treatment of lung cancer forward Technologies such as VATS, EBUS/EUS and mediastinoscopy are critical in this endeavor