Download
1 / 36
560 likes | 2.08k Views
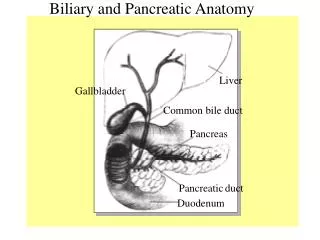
Percutaneous Transhepatic Cholangiography and Biliary Intervention. Indications. Treatment of malignant obstruction Adjunct to surgery Treatment of CBD calculi Treatment of benign strictures Diagnostic? Failed ERCP. Patient selection. WHO performance status Imaging

E N D
Percutaneous TranshepaticCholangiography andBiliary Intervention
Indications • Treatment of malignant obstruction • Adjunct to surgery • Treatment of CBD calculi • Treatment of benign strictures • Diagnostic? • Failed ERCP
Patient selection • WHO performance status • Imaging • Clinician/MDT discussion • Coagulation status • Ascites
WHO performance status • 0 – 2. • In bed less than 50% of time • BSIR Audit report 2009, 19.8% in hospital mortality • 15.6% in hospital mortality for benign disease • Audit of my procedures, 18% 30 day mortality • Patients with lower WHO performance status do better
Imaging • Ultrasound. Confirm biliary obstruction, mass, metastatic disease, calculi • CT. Confirm level of obstruction, mass, metastatic disease • MRI/MRCP. Complex biliary strictures, CBD calculi, liver metastases • ERCP. May have failed
Clinician/MDT discussion • Malignant or benign disease • Gastroenterologists • Surgeons • Radiologists • Other Healthcare Workers
Malignant Disease • Surgical. ERCP and plastic stent or PTC and Internal/External biliary drainage • Palliative. ERCP or PTC and metallic Stent
Benign Disease • ERCP treatment of choice • PTC and internal/external drain or plastic stent. May enable successful ERCP later
Coagulation status • INR < 1.4. Consider vitamin K, FFP and also Beriplex/Octaplex. Contain prothrombin complex concentrate. Factors II, VII, IX and X as well as Proteins C and S • Platelets > 100,000. If less, consider platelet transfusion
Consent • WHO performance status • Check coagulation • Explain procedure at least 1 day before • Risks. Bleeding, bile leak, infection, pneumothorax and failure
Anaesthetic • Anaesthetist • GA • Discuss need for airway protection • Use LA • When applying for consultant post ask what access you may have to anaesthetics
Antibiotics • At start of procedure • Gentamicin 240 mg IV • Metronidazole 500 mg IV • Discuss with Microbiology
Equipment • Use what works best for you • Chiba needle 22 gauge • Trochar needle 18 gauge • NEF set • Stiff Terumo wire • Amplatz wire • Catheters. BMC and straight • Self expanding stent • Internal/External drains 8.5/10.5F. Discuss with your surgeon
Approach/Technique 1 • Ascites present? Drain first • Ultrasound? • Right lobe. Mid axillary line. Aim for xyphisternum. • Left lobe. Locate with U/S and usually aim for segment III. • Very gently inject 1/3 strength contrast (100) as needle is withdrawn • Duct entered when contrast flows away from needle and persists • Duct not entered. Change angle and try not to exit liver capsule • Duct normally anterior to portal vein
Approach/Technique 2 • Pre-surgery for cholangiocarcinoma. Discuss lobe to drain. Usually the lobe being preserved. • Pre-surgery for pancreatic cancer. Right lobe puncture. • Palliative. Drain right, left or both? • 1. Chiba needle to opacify ducts then choose duct for trochar puncture and wire etc. • 2. NEF set. Single puncture then wire, dilator and access sheath • Consider bile for cytology if no diagnosis
Approach/Technique 3 • Stiff Terumo to cross lesion. Use pin vice for torque • Straight catheter • Amplatz wire • Dilator • Stent/Drain • 1 or 2 stage procedure? • Temporary drain following stent? • Plug track? Coils, gelfoam etc. • Technical success >95% (BSIR audit)
Approach/Technique 4 • Unable to cross stricture, establish external drainage (8.5F internal/external drain). Further attempt after decompression usually successful. Care with drainage bag essential. • Internal external drainage, try not to use bag and bung catheter.
BSIR Audit. Mortality & Complications (reported) • In hospital mortality 19.8%. • Death or major complication 21.2% overall, 18.3% benign, 21.7% malignant. • Major complications in 7.9%, haemorrhage 3.5%, renal failure 1.8% and sepsis 1.6%. • Minor complications in 26.0%, pain 14.3%, sepsis 7.7% and haemorrhage 4.5%. • Association with ascites, elevated INR and low platelets. • 1 year survival <20% for malignant disease. • Drainage more effective if stents placed across ampulla
BSIR recommendations • 1. Further audit of this cohort is required to determine cause of death and to demonstrate whether or not there are significant associated risk factors. • 2. Given the high mortality in this group of patients further data collection will be required. Significant improvements in data completeness are required. Data submission remains voluntary, but NHS services should consider how they can make resources available to support data collection for individual operators
Case 1 • 86 yr female presented with sepsis and subsequent jaundice • Arteriopath but otherwise reasonably fit • CT
Case 1 • Abscess right lobe liver drained • Antibiotics • MDT discussion, for palliation • ERCP, failed to stent due to large duodenal diverticulum • PTC
Case 2 • 69 yr male with obstructive jaundice • CT, operable mass in head of pancreas • MDT discussion • Surgical candidate • ERCP to place plastic stent failed • PTC
Case 3 • 75 yr female with obstructive jaundice • CT, large central liver mass, likely cholangiocarcinoma. Further deposit in segment II • MDT discussion, not operable, palliative • PTC and stent left lobe
Case 4 • 71 yr male • Metastatic colorectal cancer • Multiple liver resections • Jaundice with recurrent liver and peritoneal tumour • Considering further chemotherapy • CT Small residual liver with mild duct dilatation • ERCP failed
Case 5 • 59 yr female with inoperable cholangiocarcinoma • Previous ERCPs with plastic and finally recently metal stent into left lobe • Recurrent jaundice • ?percutaneous options
Take Home Points • Careful patient selection after MDT discussion • “Appropriate” Anaesthesia • Try not to use external drainage bags