Download
1 / 12
120 likes | 448 Views
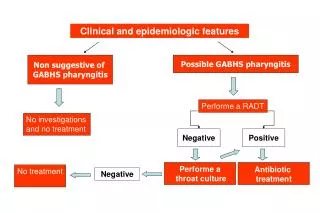
CLINICAL FEATURES. Initial Symptoms in Patients with Meningitis Headache 90 % Fever 90 % Meningismus 85 % Altered sensorium >80 % Kernig's Brudzinski's sign 50 % Vomiting 35 % Seizure 30 %. Meningitis: CSF profile.

E N D
CLINICAL FEATURES • Initial Symptoms in Patients with Meningitis Headache 90 % Fever 90 % Meningismus 85 % Altered sensorium >80 % Kernig's Brudzinski's sign 50 % Vomiting 35 % Seizure 30 %
DIAGNOSIS - Cerebrospinal Fluid Examination • The CSF in cases of acute bacterial meningitis often demonstrates a purulent (cloudy) appearance and contains large numbers of neutrophils (5,000 to 10,000 per cubic millimeter of CSF). In addition, the protein is usually elevated and the sugar decreased. A definitive diagnosis of pyogenic meningitis depends on the demonstration of bacteria with a gram stain and/or subsequent culture. Pyogenic Meningitis Neutrophils Elevated protein Decreased sugar Positive gram stain
DIAGNOSIS - Cerebrospinal Fluid Examination • In cases of granulomatous and lymphocytic meningitis , the CSF is, in general, not cloudy and the cellular infiltrate consists of lymphocytes, although the CSF may contain neutrophils in the early stages. As in pyogenic meningitis, the CSF protein and sugar are increased and reduced, respectively. Granulomatous &Viral Meningitis Lymphocytes Elevated protein Decreased sugar Negative gram stain
INITIAL MANAGEMENT OF PATIENTS WITH ACUTE MENINGITIS • The initial management of a patient with presumed bacterial meningitis includes performance of a lumbar puncture to determine whether the CSF formula is consistent with that diagnosis • If purulent meningitis is present, institution of antimicrobial therapy should be based on the results of Gram staining or rapid bacterial antigen tests. • However, if no etiologic agent can be identified by these means or if performance of the lumbar puncture is delayed (i.e., longer than 90 to 120 minutes), institution of empirical antimicrobial therapy should be based on the patient's age and underlying disease status.
Recommended Antimicrobial Therapy for Acute Bacterial Meningitis Based on the Presumptive Pathogen Identified by Positive Gram Stain or Bacterial Antigen Test • Haemophilus influenzae type B 3rd-gen cephalosporin • Neisseria meningitidis Penicillin G or ampicillin • Streptococcus pneumoniae Vancomycin plus a 3rd-gen cephalosporin • Listeria monocytogenes Ampicillin or penicillin G • Streptococcus agalactiae Ampicillin or penicillin G • Escherichia coli 3rd-gen cephalosporin
Empirical Therapy for Purulent Meningitis 0-4 wk Ampicillin plus cefotaxime; or ampicillin plus an aminoglycoside 4-12 wk Ampicillin plus a third-gen cephalosporin 3 mo to 18 yr Third-generation cephalosporin ; or ampicillin plus chloramphenicol 18-50 yr Third-generation cephalosporin >50 yr Ampicillin plus a third-gen cephalosporin
Empirical Therapy for Purulent Meningitis • Immunocompromised Vancomycin + ampicillin + ceftazidime • Basilar skull fracture Third-generation cephalosporin • Head trauma Vancomycin plus ceftazidime • Postneurosurgery Vancomycin plus ceftazidime • Cerebrospinal fluid shunt Vancomycin plus ceftazidime • The duration of antimicrobial therapy in patients with bacterial meningitis has been 10 to 14 days for cases of nonmeningococcal meningitis. Meningococcal meningitis can be treated for 7 days with intravenous penicillin.
Therapy for Viral Meningitis • Treatment of acute viral encephalitis and meningitis (except herpes) is directed at symptom relief, supportive care, and prevention and management of complications. • Although seizures sometimes complicate encephalitis, prophylactic anticonvulsants are not routinely recommended. • If seizures develop, they can usually be managed with phenytoin and phenobarbital. • Steroids should probably generally be avoided in the treatment of encephalitis because of their inhibitory effects on host immune responses. • Full recovery from viral meningitis usually occurs within 1 to 2 weeks of onset
Therapy for Meningitis • In patients who present with focal neurologic findings or who have papilledema and bacterial meningitis is suspected, a CT scan of the head should be performed before lumbar puncture to rule out the presence of an intracranial mass lesion because of the potential risk of herniation. • After obtaining blood cultures, the emergency empirical antimicrobial therapy should be initiated before sending the patient to the CT scanner. • Once the infecting meningeal pathogen is isolated and susceptibility testing known, antimicrobial therapy can bemodified for optimal treatment.
Therapy for Meningitis • In addition, certain patients should receive adjunctive dexamethasone therapy when presenting with suspected or proven bacterial meningitis . • Currently, data support the routine use of adjunctive dexamethasone therapy (0.15mg/kg every 6 hours for 2 to 4 days) in infants and children with meningitis caused by H. influenzae type B • In adults or in patients with meningitis caused by other bacteria, dexamethasone is not routinely recommended, although some authors recommend its use in all patients with presumed bacterial meningitis.