Download
1 / 35
460 likes | 1.06k Views
Shock: Clinical features and pathophysiology. Mahesh Nirmalan Critical Care Unit, Manchester Royal Infirmary. Objectives. Life-threatening condition Immediate or delayed mortality Multiple aetiology Recognition and Assessment Physiological consequences of shock clinical features

E N D
Shock: Clinical features and pathophysiology Mahesh Nirmalan Critical Care Unit, Manchester Royal Infirmary
Objectives • Life-threatening condition • Immediate or delayed mortality • Multiple aetiology • Recognition and Assessment • Physiological consequences of shock • clinical features • Document and report on progression
Definition of Shock • Inadequate tissue perfusion • Decreased oxygen supply • Anaerobic metabolism • Accumulation metabolic waste
Causes of Shock • Severe or sudden blood loss • Large drop in body fluids • Myocardial infarction • Major infections • High spinal injuries • Anaphylaxis • Extreme heat or cold
Types of Shock • Hypovolemic Shock: • haemorrhagic • or non haemorrhagic • Other causes of shock • Cardiogenic Shock • Septic Shock • Neurogenic Shock • Anaphylactic Shock
Hypovolaemic Shock • Haemorrhage: Overt or occult • Reduction in circulating volume • Reduction in venous return and CO • O2 supply-demand imbalance • Lactic acidosis • Reduction in venous oxygen saturation • Non haemorrhagic hypovolaemia • Severe burns, vomiting and diarrhoea
% Blood loss Clinical Signs < 15 Slightly increased heart rate, local swelling, bleeding 15-30 Increased heart rate, increased diastolic blood pressure, prolonged capillary refill 30-50 Above findings plus: hypotension, confusion, acidosis, decreased urine output > 50 Refractory hypotension, refractory acidosis, death Clinical Signs of Acute Hemorrhagic Shock
Signs of Shock • Cold, clammy and pale skin • Rapid, weak, thready pulse • Shallow, rapid breathing • Oliguria • Reduction in MAP • Cyanosis • Loss of consciousness
Non-Haemorrhagic Shock • Cardiogenic Shock • Septic Shock • Neurogenic Shock • Anaphylactic Shock
Cardiogenic Shock • Primary myocardial failure • Arrhythmia • Tamponade • Contusion • Pump failure • Reduction in cardiac output: • Decreased blood supply • Decreased oxygen delivery
Cardiogenic Shock • Assess for: • Signs of heart failure • Signs of tamponade • Cardiac dysrrhythmia • Myocardial infarction • Tachycardia • Muffled heart sounds or third heart sound • Engorged neck veins with hypotension • Dyspnoea • Oedema in feet and ankles
Septic Shock • Bacterial, viral, fungal infection • Gram negative and gram positive bacteria • High output failure: “warm shock” • Fever, tachycardia, tachypnoea, leucocytosis • Inadequate oxygen extraction • High SvO2, Metabolic acidosis • “Cold shock” • Atypical presentation in immuno-compromised patients • Diabetes, Cirrhosis, immunosuppression
Septic Shock in trauma patients • Develops 2 - 5 days after injury occurs • Carries a poor prognosis • Assess for: • Penetrating abdominal injuries • Signs of infection • Warm pink skin and dry elevated body temperature • Tachycardia • Wide pulse pressures
Neurogenic Shock • Caused by: • Spinal cord injury • Certain drugs • Brain stem, spinal or torso trauma • Venous pooling and arteriolar dilatation • Signs and Symptoms: • Hypotension without tachycardia • Warm pink skin • Low blood pressure & minimal response to fluids
Anaphylactic Shock • Rapid onset • Primary systems: • Cardiovascular, Respiratory • Skin, Gastrointestinal, coagulation • Face, pharynx and laryngeal oedema • Adrenaline is life saving
Anaphylactic Shock • Diffuse vasodilatation • Increase size of vascular bed • Blood is trapped in small vessels and viscera • Temporary loss in total circulatory volume • Sudden severe allergic reaction to: • Drugs, Toxins, Foods, Plants
Symptoms • Apprehension and flushing • Wheezing or shortness of breath & cough • Rapid, weak pulse • Cyanosis • Generalized itching or burning • Watering and itching of the eyes • Hypotension • Coma
Stages of shock • Compensated shock • Autotransfusion • Decompensated shock • Blood moves to more vital organs • Irreversible shock • Multiple system / organ damage • Even with treatment, death is the result
Plasma [Lactate] A priori groups Post hoc groups
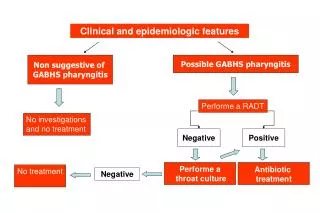
Evaluation of Shock • Internal or external hemorrhage • Underlying cardiac problems • Sepsis • Trauma to spine cord • Contact with known allergic substance • Determine amount of blood loss • How long has casualty been bleeding?
Level of Consciousness Report and record • Alert • Verbal response to stimuli • Pain response to stimuli • Unresponsive to any stimuli
Early Signs of Shock in Non Complicated Patients • High index of suspicion • Minimum tachycardia • No measurable changes occur in blood pressure • Pulse pressure is potentially very useful
Definitive management Where? By whom?
Invasive monitoring • Essential in the definitive treatment • Direct arterial pressure • Central venous pressure • Cardiac output
Treatment of Shock • Maintain airway • Control bleeding • Baseline vital signs • Level of consciousness Increase tissue perfusion and oxygenation status
Treatment of Shock • Positioning • ABCD approach • Fluid therapy • Drug therapy • Keep patient at normal temperature • Prevent hypothermia • Minimize effect of shock • On-going assessment - every 10-15 minutes
Specific measures • Hypovolaemia: Blood transfusion • Electrolyte/acid base imbalance • Sepsis: Antibiotics, ?steroids • Neurogenic: Steroids • Anaphylactic: Adrenalin
Summary • Life threatening: Early goal directed therapy and regular monitoring by trained staff will change outcome. • Early detection : DON’T RELY ON BP • High index of suspicion • Monitor casualties susceptible to shock