Download
1 / 39
390 likes | 554 Views
The “Right” Way to Insert a Shunt. James M. Drake FRCSC. The Hospital for Sick Children University of Toronto, Canada. Consensus Conference on Clinical Hydrocephalus in Children September 20, 2013. Please note: James Drake, MD Will discuss commercial products or services.

E N D
The “Right” Way to Insert a Shunt James M. Drake FRCSC The Hospital for Sick Children University of Toronto, Canada
Consensus Conference on Clinical Hydrocephalus in ChildrenSeptember 20, 2013 Please note: James Drake, MD • Will discuss commercial products or services. • Will discuss non-FDA approved uses of products/providers of services. • Has financial arrangements or affiliations with: MDA Robotics – in kind grant support related to surgical robotics L3 Communications – in kind grant support related to surgical simulation Phillips Medical Imaging – in kind grant support related to MR imaging focused ultrasound Medical Modelling – licensing fee for research support related to craniofacial modelling
Lineage - + ? Shunt Surgery: a passion, demand for excellence
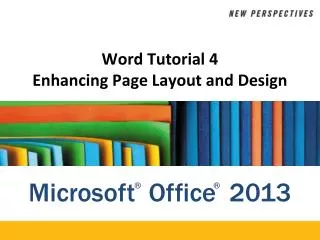
1.0 Repeated Shunt Failure Survival Analysis 834 patients, 1181 procedures .8 1st Failure 2nd Failure 3rd Failure .6 4th Failure Proportion Shunt Failure Free .4 .2 0.0 1000 2000 3000 4000 Follow up (Days)
The influence of surgical operative experience on the duration of first ventriculoperitoneal shunt function and infection.Cochrane DD, Kestle JR.Pediatr Neurosurg. 2003 Jun;38(6):295-301 The relationship of surgeon experience, measured by operative volume, to the outcomes of ventricular shunt treatment of hydrocephalus in children is not clear. This paper explores this relationship based on first ventriculoperitoneal shunts (VPS) implanted in English-speaking Canada during the period from April 1989 to March 2001. Three thousand seven hundred and ninety-four first VPS insertions, performed by 254 surgeons, were reviewed. Surgical experience was represented by the number of shunt operations performed during the study period by each surgeon prior to the date of the operation. The 6-month shunt failure risk for less experienced surgeons was 38%, compared to 31% for more experienced surgeons. This difference decreased to 4% at 60 months and 3% at 120 months (p = 0.001). The infection rate for initial shunt insertions was 7% for patients treated by more experienced surgeons and 9.4% for those treated by less experienced surgeons (p = 0.006). A relationship between surgeon experience and shunt outcome that appears to be based on the operative experience that a surgeon brings to a procedure is in keeping with clinical experience. This observation has implications for public policy, service planning and surgical mentorship during the earlier years of a surgeon's career.
In-hospital mortality rates after ventriculoperitoneal shunt procedures in the United States, 1998 to 2000: relation to hospital and surgeon volume of care.Smith ER, Butler WE, Barker FG 2nd.J Neurosurg. 2004 Feb;100(2 Suppl):90-7Neurosurgical Service, Massachusetts General Hospital, Boston, Massachusetts 02114, USA.OBJECT: Death after ventriculoperitoneal (VP) shunt surgery is uncommon, and therefore it has been difficult to study. The authors used a population-based national hospital discharge database to examine the relationship between annual hospital and surgeon volume of VP shunt surgery in pediatric patients and in-hospital mortality rates. METHODS: All children in the Nationwide Inpatient Sample (1998-2000, age 90 days-18 years) who underwent VP shunt placement or shunt revision as the principal procedure were included. Main outcome measures were in-hospital mortality rates, length of stay (LOS), and total hospital charges. Overall, 5955 admissions were analyzed (253 hospitals, 411 surgeons). Mortality rates were lower at high-volume centers and for high-volume surgeons. In terms of hospital volume, the mortality rate was 0.8% at lowest-quartile-volume centers (< 28 admissions/year) and 0.3% at highest-quartile-volume centers (> 121 admissions/year). In terms of surgeon volume, the mortality rate was 0.8% for lowest-quartile-volume providers (< nine admissions/year) and 0.1% for highest-quartile-volume providers (> 65 admissions/year). After multivariate adjustment for demographic variables, emergency admission and presence of infection, hospital volume of care remained a significant predictor of death (odds ratio [OR] for a 10-fold increase in caseload 0.38; 95% confidence interval [CI] 0.18-0.81). Surgeon volume of care was statistically significant in a similar multivariate model (OR for a 10-fold increase in caseload 0.3; 95% CI 0.13-0.69). Length of stay was slightly shorter and total hospital charges were slightly higher at higher-volume centers, but the differences were not statistically significant. CONCLUSIONS: Pediatric shunt procedures performed at high-volume hospitals or by high-volume surgeons were associated with lower in-hospital mortality rates, with no significant difference in LOS or hospital charges.
Is there a ‘July Effect’ Affecting Shunt Survival? Revisiting this Issue Using Prospectively Collected Data from the HCRN’s Shunt Registry. Riva-Cambrin, Kestle, Whitehead, Browd, Holubkov, Drake, Limbrick, Tamber, Rozelle, Simon, Wellons, Kulkarni for the HCRN Introduction: The ‘July Effect’ is the notion that hospital services see a spike in complications in July and August, presumably from annual turnover of new housestaff. Previous reports were contradictory and this issue has important ramifications for patient care, resident training, and clinical performance metrics. Methods: The HCRN Shunt Registry was examined for first shunt placements in children aged less than 19 years at 6 of the 7 HCRN sites. Shunt failure was defined as shunt revision or shunt infection. The independent variable at study was the calendar month in which the first shunt was placed. The Cox proportional hazard regression modeling included risk adjustment for age, etiology, cardiac co-morbidity, endoscope use, and shunt hardware. Results: 1036 children underwent first shunt placement from April 2008 to December 2011. 344 patients had shunt failure including 265 malfunctions and 79 infections. Of shunts placed in July and August, 32.0% failed during follow-up versus 33.4% placed during all other months combined (p=0.80). Infections of shunts placed during July and August trended non-significantly lower (4.6%) versus 8.3% inserted the other months (p=0.08). In multivariable regression, shunts insertion in July or August was not associated with failure (p=0.75), whereas age, cardiac co-morbidity, and use of the endoscope remained significant, as previously reported by the HCRN. Conclusions: We found no evidence to support a ‘July Effect’ in first shunt surgeryusing a large multi-centered cohort derived from the HCRN Shunt Registry with or without risk adjustment for known confounders.
UK Shunt Registry 1615 patients
There is no such thing as a “routine” shunt procedure • Noted to be pale cyanotic following intubation. • Cannot get blood pressure, sinus tacchycardia • Have venous access, try and establish more, no success. • Call code. Specifically call ICU staff for assistance • No obtainable blood pressure, Full code with CPR commenced 2 mos Dandy Walker Massive scalp swelling post EVD insertion • Code lasts 1 hour 40 minutes • Dopamine drip, then epinephrine drip • 16 epinephrine boluses; 11 Na Bicarb ; 6 Ca Cl • Intraoperative ultrasound of head, which is now tense, clearly expanding, massive bleeding into subdural spaces • Pt receives Albumen, Blood (12 boluses of ~ 20 cc - 2 units), 3 boluses platletts, 5 boluses of FFP. • Still active bleeding clinically, and on ultrasound • I suggest activated Factor VII. Call heamatology – no idea, call thrombosis, no idea, call blood bank “routine blood product” send to OR. Package arrives, no one any idea of how to mix it. Read directions inject, patient stabilizes within 10 minutes • Intraoperative echo, hypovolemia, no tamponade. • Patient receives 1 hour 20 minutes of chest compressions. Has eyes open and moving at ~ 1 hour point. Leaves OR moving all 4. • Parents return from Santa Claus parade
Shunt Insertion Rule Book • Take the shunt procedure seriously – error intolerant • Plan the operation appropriately - vent size, skin, lines, trach, etc • Use devices you are familiar with • Consider using guidance for catheter placement, laparoscopy for abdomen • Nothing less than perfect surgical technique is acceptable
Anterior Shunt v. Posterior Shunt Survival Curves (unadjusted) Log rank test, p<0.0001 Whitehead et al.
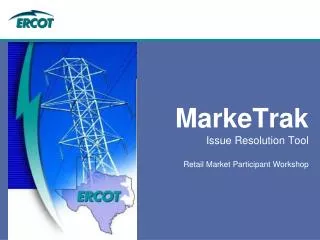
frontal body occipital Imaging Analysis Shunt Design Trial344 patients, up to 6 scans eachventricular catheter tip location, environment* Surrounded by CSF Touching Brain Surrounded by Ventricle * Failure scans excluded
J Neurosurg. 2007 Nov;107(5 Suppl):406-10. Accurate placement of cerebrospinal fluid shunt ventricular catheters with real-time ultrasound guidance in older children without patent fontanelles. Whitehead WE, Jea A, Vachhrajani S, Kulkarni AV, Drake JM.
Ultrasound Guided Shunt Insertion Does Not Significantly Improve the Rate of Accurate Ventricular Catheter Placement: A Prospective, Controlled Study by the Hydrocephalus Clinical Research Network (HCRN) William E. Whitehead, MD;1Jay Riva-Cambrin, MD, MSc;2John C. Wellons III, MD, MSPH;3Abhaya V. Kulkarni, MD, PhD;4 Richard Holubkov, PhD;2Anna Illner, MD;1 W. J. Oakes, MD;5Thomas G. Luerssen, MD;1 Marion L. Walker, MD;2James M. Drake, FRCSC;4 and John R. W. Kestle, MD;2 for the Hydrocephalus Clinical Research Network. Table 6: Shunt Outcomes at 1 Year
Accurate placement of the ventricular catheter reduces the shunt failure rate ?
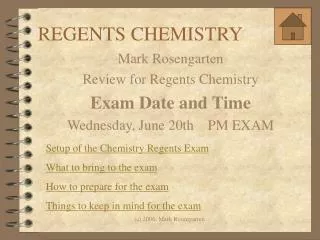
Shunt survival in endoscope ( ) and non endoscope ( ) groups 376 patients Proportion of shunts functioning (N = 393, log rank = 2.92, p = 0.09) Time (years) Kestle, Drake, Cochrane et al, J Neurosurgery, 2003
Tricks of the TradeVentricular catheter • The dural opening should be snug • There should be brain to “grab” the catheter, if not use a right angle connector • The catheter should be long, especially in neonates – growth will pull it out • Take care with connector – can tear the tubing, and make sure the circlage suture indents the tubing, knot underneath
Conclusions • Probably most important issue with the technique of shunt insertion is to pursue excellence • The improved results from more experienced, or pediatric neurosurgeons are small but significant. • These small differences become large with increasing number of patients. • Adjuncts such as ultrasound, laparoscopy probably help but are hard to prove. • Be prepared to change based on new evidence.