Download
1 / 37
380 likes | 494 Views
Assessing the Cost of VistA/EHR Building a business case with ROI. Claudine D. Beron, PMP March 2, 2007. VistA Project Life Cycle.

E N D
Assessing the Cost of VistA/EHRBuilding a business case with ROI Claudine D. Beron, PMP March 2, 2007
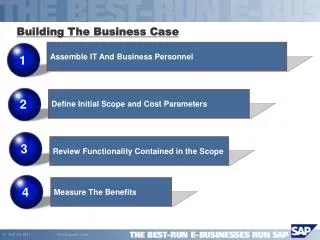
VistA Project Life Cycle Project Management for VistA is accomplished through the use of the core areas including: initiating, planning, executing, controlling, and closing and represents over 44 processes from PMI. Initiate Plan Close Execute/Control Assess • Environment • Needs • Standard Operating Procedures • Benefits • Resources Strain • Budget Accept • Identify Owners • Identify Stakeholders • Future Budgeting • Complexity Deploy • Hardware • Software • Configure to Environment Educate • Compare EHRs • Build Business Case • Develop ROI • Understand Functionality Train • Ongoing maintenance • Clinical Staff Support • Ongoing maintenance • Updates/Patches • Additional modules
+ Cash Flow Impact - Time What is Business Case Analysis? • Definition: a forecast of the financial impact, over time, of a decision – typically an investment, capital purchase, or project • A full Business Case analysis forecasts the project costs, benefits, and the timing of both elements • Results may be expressedas a time series (see graphic)or summarized by a singlefinancial metric Mark Leavitt, MD, PhD, FHIMSS. Case for EHR in Small Physician Offices - Physician Office QIOSC National Call -- January 11, 2005
+ Net Cash Flow - Time Financial Metrics NPV • Net Cash Flow • How much extra cash will this costor generate for our business eachmonth / quarter / year? • Well-suited to the medical practice,where ‘cash (flow) is king’ • Discounted Cash Flow • Like Net Cash Flow, but adjustedfor ‘time value’ of money • Net Present Value • Sums up the discounted cash flows to give a single value • Payback Period • How long until project ‘pays for itself’ • Good measure of relative risk: long payback = high risk • Internal Rate of Return (IRR) • Compares investment with an interest-bearing note • Not well suited to measure an IT project – buying a bond vs. implementing an EHR couldn’t be more different! IRR Payback Period Mark Leavitt, MD, PhD, FHIMSS. Case for EHR in Small Physician Offices - Physician Office QIOSC National Call -- January 11, 2005
Business Case Analysis for EHR Lumetra. EHR - Estimated Cost Savings Worksheet with additional inputs from Claudine Beron on implementation of VistA at 7 site facility
Business Case Analysis for EHR Lumetra. EHR - Estimated Cost Savings Worksheet with additional inputs from Claudine Beron on implementation of VistA at 7 site facility
Business Case Analysis for EHR Lumetra. EHR - Estimated Cost Savings Worksheet with additional inputs from Claudine Beron on implementation of VistA at 7 site facility
Business Case Analysis for EHR Lumetra. EHR - Estimated Cost Savings Worksheet with additional inputs from Claudine Beron on implementation of VistA at 7 site facility
Relationship of RIO and Complexity of Environments Lynn Harold Vogel, PhD. Finding Value from IT Investments: Exploring the Elusive ROI in Healthcare. Journal of Healthcare Information Management — Vol. 17, No. 4. October 14, 2003
Common Approaches to ROI • The common approach to VistA: • 1. Identify the business processes affected by IT – these are all the standard operating procedures for the hospital, clinic or physician office • 2. Estimate current costs per transaction – estimate $1 per pull of each hardcopy file • 3. Estimate future cost per transaction after IT investment – estimate $.10 cents per transaction • 4. Estimate the net yearly cost savings – based on # of queries and patient bed size
Overview of Proposed Method • Gather Objective Data. Gather information on cost of IT, use of IT and revenues of the organizational unit or the entire organization. Gather data on at least three longitudinal time periods or three cross-sectional units of organization within one time period. • Verify Expected Associations. If returns can be attributed to IT investment, there must be an association among cost of IT, use of IT and revenues. • Verify Causality. Test whether increased revenue has led to more IT use or vice versa. • Calculate ROI. If IT investment can be assumed as the reason for growth in revenue, calculate a rate of return.
Gather Objective Data • Gather information on cost of IT, use of IT and revenues of the organizational unit or the entire organization. Gather data on at least three longitudinal time periods or three cross-sectional units of organization within one time period. • Current – paper based office/clinic/hospital • Fixed • Salaries, Fringe, etc. • Office Supplies (Files, paper etc.) • Storage (cabinets, room space and off-site) • Legacy support • Variable • Patient error rates • Lost records • Illegible records
Verify Expected Associations • If returns can be attributed to IT investment, there must be an association among cost of IT, use of IT and revenues. • VistA Cost of IT • Hardware, Software, peripherals, printers • Assessment and Change of Business Process Reengineering • Legacy support, interfacing, transition • On going Training for Clinical and Technical support • Use of IT – Why change? • Improved Patient Safety • Reduce personnel cost • Manage shortages of Nursing staff • Revenue? • Do you intend on providing more services? • Will the change impact revenue stream?
Verify Causality • Test whether increased revenue has led to more IT use or vice versa • Increased Revenue • Is this system adding to revenue? If not, when? • Use • Are Doctors and Nurses using the System or are they reverting back to old system?
Healthcare Market Segments • The healthcare market has been categorized into four distinct segments. The four categories are: • Market Segment 1: Hospital and Hospice Services • Market Segment 2: Community Hospitals • Market Segment 3: Medical Centers • Market Segment 4: Health Networks
Market 1 Hospital and Hospice Care This market segment is defined by organizations that provide general inpatient care and hospice services. The workforce is composed of clinicians that frequently practice within local areas. Clinicians are supported by skilled full time employees. These facilities rely upon a composite of consulting professionals and partnerships with larger hospitals. Organizational structures are flat with individuals performing several roles. * American Hospital Association Survey (USA Only): 2003
Market Profile 1 Hospital and Hospice Care These organizations are frequently challenged by health information management. Narrow sources of funding and revenue constraints dictate efficient care documentation for reimbursement, regulatory compliance and provider coordination. IT solutions should focus on core segments of clinical workflow. This market segment seeks solutions that are quickly implemented, highly supported and require limited customization. Stakeholders require that solutions enhance operations while allowing organizational attention to remain upon patient care. Vendors must offer full automation of the documentation with an integrated health data repository. Automated medication administration, transcription entry, results viewing and scheduling. The implementation of solutions should center upon small cross-trained teams on-site for brief periods. This team should then be supported by remotely located associates for limited software customization, workflow design, training and adoption management services. Hardware solutions should focus upon remote hosting solutions.
Market 2 Community Hospitals The market segment is defined by small community hospitals that provide general practice care to communities within a region. The clinical workforce is stable with low turnover and is composed of full time physicians and support staff. The facilities serve as a central base for medical services in support of area clinics and community based care. * American Hospital Association Survey (USA Only): 2003
Market Profile 2 Community Hospitals The dominant challenges of these organizations is the centralization of health information, staff productivity, treatment coordination and financial management. Departments require access to patient treatment information to standardize and communicate patient care. Emphasis is placed upon departmental specific functionality. Treatment documentation must enhance productivity while facilitating revenue capture. Vendor solutions should focus on disciplinary workflow, orders management, results/image viewing, financial management and automated interdepartmental workflow. Stakeholders value process re-design and comprehensive IT support that establishes internal expertise. The implementation teams should work on-site for limited periods to collect data on workflow design, software customization, stakeholder engagement and training. Hardware solutions should offer on-site solutions only.
Market 3 Medical Centers The market segment is defined by large hospitals within metropolitan areas. A full spectrum of patient care is offered. These facilities have frequently undergone merger and integration into regional health networks. Segments of the clinical workforce are prone to turnover and are defined by specialized areas of expertise. Extensive provider partnerships are formed to offer patients comprehensive services. Management organization is hierarchal with specialized support departments. Executive stakeholders value scaleable technology with vision. * American Hospital Association Survey (USA Only): 2003
Market Profile 3 Medical Centers Organizations within this segment are focused upon streamlining workflow within departments, standardization of care, integration of treatment data and the automation of financial information. The highly siloed departments within these organizations challenge the standardization and continuity of care across organizational boundaries. Frequent bottlenecks occur in the communication and formatting of treatment and financial data. Merger processes frequently cause fragmentation of organizational processes. Vendor solutions should focus upon solutions that standardize and automate discipline specific workflow across departments and facilities. A centralized data repository with a standardized user interface must be accessible regardless of location. Departmental hardware must be interfaced to an EHR solutions for automated data capture. The implementation approach should utilize a team of specialized clinical experts and project management on-site for extended periods to perform workflow design, system customization and configuration and adoption management services.
Market 4 Health Networks The market segment is defined by full spectrum health centers that are regionally and nationally for specific areas of clinical excellence. These providers are organized within large health maintenance networks and teaching organizations. The hierarchal organization contains significant specialization within clinical and support silos. Turnover of staff is significant due to teaching functions and the broad lines of business within competitive markets. * American Hospital Association Survey (USA Only): 2003
Market Profile 4 Health Networks Organizational challenges center around the competing objectives within the large hospital departments. Departmental siloes fragment workflow across departments. This results in the constriction of patient treatment information, continuity of care and standardization of processes. IT focus is placed upon solutions that seamlessly transmit data and automate interdepartmental workflow. Integrated solutions must demonstrate the flexibility to address multiple departmental objectives such as capturing charges while facilitating teaching and care documentation. Stakeholders require that solutions address workflow issues within the framework of a clear return on investment model. These organizations prefer to own initiatives with internal IT expertise. Vendors must present a scaleable technological vision with clear implementation and change management strategies.
Contacts Claudine Beron, PMP Accenture, LLP 703-947-3610 703-599-1203 cell claudine.d.beron@accenture.com
VistA Links VistA-CPRS Demo - http://www1.va.gov/CPRSdemo/ CMS - VistA Office EHR – http://www.cms.hhs.gov/quality/pfqi.asp#Vista-Office%20EHR Indian Health - RPMS - http://www.ihs.gov/Cio/RPMS/index.cfm DoD - CHCShttp://www.tricare.osd.mil/peo/citpo/projects.htm Pacific Hui - http://www.pacifichui.org/ WorldVistA - http://www.worldvista.org Hardharts.org - http://www.hardhats.org/ Vista Software Alliance- http://www.vistasoftware.org
VistA Article Links • VistA - U.S. Department of Veterans Affairs National Scale Healthcare Information Systems (HIS), International Journal of Medical Informatics, February, 2003. • http://www1.va.gov/cprsdemo/docs/VistA_Int_Jrnl_Article.pdf • The Veterans Health Administration: Quality, Value, Accountability, and Information as Transforming Strategies for Patient-Centered Care , The American Journal of Managed Care, November, 2004. • http://www1.va.gov/cprsdemo/docs/AJMCnovPrt2Perlin828to836.pdf • Comparison of Quality of Care for Patients in the Veterans Health Administration and Patients in a National Sample , Annals of Internal Medicine, December, 2004. • http://www1.va.gov/cprsdemo/docs/Internal_Medicine_Article_on_VistA.pdf • The Best Care Anywhere , Washington Monthly, January/February, 2005 • http://www1.va.gov/cprsdemo/docs/Article_Washington_Monthly_Jan_Feb_2005.doc
VistA Reading • West; O’Mahony, “Contrasting Community Building in Sponsored and Community Founded Open Source Projects,” Proceedings of the 38th Annual Hawai‘I, International Conference on System Sciences, Waikoloa, Hawaii, January 3-6, 2005. http://opensource.mit.edu/papers/westomahony.pdf • Goldstein, Ponkshe, Maduro, “Profile of Increasing Use of OSS in the Federal Government and Healthcare” http://www.medicalalliances.com/downloads/files/Open_Source_Software-Government_and_Healthcare_White_Paper-Medical_Alliances_2.doc • The Veterans Health Administration: Quality, Value, Accountability, and Information as Transforming Strategies for Patient-Centered Care , The American Journal of Managed Care, November, 2004. http://www1.va.gov/cprsdemo/docs/AJMCnovPrt2Perlin828to836.pdf • Comparison of Quality of Care for Patients in the Veterans Health Administration and Patients in a National Sample , Annals of Internal Medicine, December, 2004. http://www1.va.gov/cprsdemo/docs/Internal_Medicine_Article_on_VistA.pdf • The Best Care Anywhere , Washington Monthly, January/February, 2005. http://www1.va.gov/cprsdemo/docs/Article_Washington_Monthly_Jan_Feb_2005.doc • Brown, Lincoln, Groen, Kolodner, “VistA – US Department of Veterans Affairs National Scale HIS,” International Journal of Medical Informatics. February 2003 http://www1.va.gov/cprsdemo/docs/VistA_Int_Jrnl_Article.pdf • Munnecke, Tom, “Personal Health: From Systems to Space,” July 19, 2002
EHR and ROI Reading • Sharpening the Case for Returns on Investment from Clinical Information Systems, Kevin Featherly, Dave Garets, Mike Davis, Pat Wise and Pat Becker http://www.longwoods.com/product.php?productid=18656&cat=465&page=1 • Medical Records in the Greater Los Angeles State Veterans Home: A Unique Opportunity to Improve Quality of care for May of 2006. Literally just scanned it, but could help us position for DC. Take a look. http://lewis.sppsr.ucla.edu/publications/studentreports/2006_TownsendEtAl.pdf#search=%22Doug%20Babcock%2C%20VHA%22 • EHR and the Return on Investment. HIMSS http://www.himss.org/content/files/EHR-ROI.pdf#search=%22EHR%20ROI%22 • Exploring the Elusive ROI in Healthcare http://www.himss.org/content/files/jhim/17-4/vogel.pdf • Value Measurement and Return on Investment for EHRs. Doug Goldstein, Peter Groen. July 2006 http://www.hoise.com/vmw/06/articles/vmw/LV-VM-08-06-19.html • Mark Leavitt, MD, PhD, FHIMSS. Case for HER in Small Physician Offices - Physician Office QIOSC National Call -- January 11, 2005 • Current Return on Investment (ROI) Literature for EHRs in Small- to Medium-Sized Physician Offices. Lumetra http://www.providersedge.com/ehdocs/ehr_articles/Current_ROI_Literature_for_EHRs_in_Small_to_Medium-Sized_Physician_Practices.pdf#search=%22Current%20Return%20on%20Investment%20(ROI)%20Literature%20for%20EHRs%20in%20Small-%20to%20Medium-Sized%20Physician%20Offices%22 • EHR Estimated Cost-Savings Worksheet. Lumetra http://www.sdfmc.org/ClassLibrary/Page/Information/DataInstances/226/Files/1176/Web_EHR_ROI_Estimated_Cost_Savings_Worksheet_Guide.pdf#search=%22EHR%20Estimated%20Cost-Savings%20Worksheet%22 • 50 Reasons to get an EHR: Quick tips from your connected colleagues will show you how EHRs change the way they work—for the better. Robert Lowes SENIOR EDITOR . http://www.cerner.com/public/filedownload.asp?LibraryID=17504