Download

1 / 16
160 likes | 246 Views
Promoting Adoption of Household Chlorination in Rural Haiti. Michael Ritter, Deep Springs International Daniele Lantagne, CDC. Jolivert Safe Water for Families Project. Began 2002 by CDC and FBO in rural Haiti MIT evaluation (2003) with 200 households after 60 weeks showed 68% correct use

E N D
Promoting Adoption of Household Chlorination in Rural Haiti Michael Ritter, Deep Springs International Daniele Lantagne, CDC
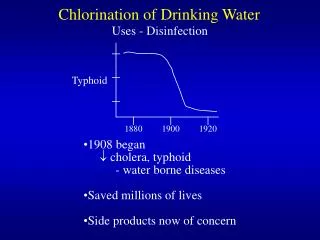
Jolivert Safe Water for Families Project • Began 2002 by CDC and FBO in rural Haiti • MIT evaluation (2003) with 200 households after 60 weeks showed 68% correct use • USAID / CDC (2005) showed 71% correct use and detailed records • Emory / CDC (2007) study on adoption • Deep Springs International now managing and replicating Jolivert project
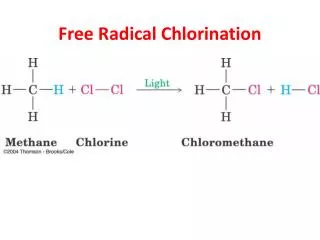
Products • Locally produced sodium hypochlorite • Refillable 240 ml bottles = 48 uses • Locally available buckets modified with tap and lid
104 communities 25 Resellers Urban Pharmacy Production Technicians at Missions of Love Clinic Rural Reseller
Methods • Analyzed longitudinal sales data for 1,709 member households • Cross-sectional randomized household questionnaire • 527 total • 357 members • 170 non-members
Avg. 76% positive Cl residual • Avg. 0.96 visits per HH per yr. (range = 0 - 7, std. dev. = 0.99) • Avg. 5.9 bottles per HH per yr.
Results **Significance p < 0.05 (mix of Chi-square, Cochran-Armitage, and Mantel-Haenzel Chi-square tests)
Conclusions and Program Recommendations • Program entry should be subsidized • Additional sales points should be established to increase convenience • Self-efficacy and social norms messages should be disseminated • Annual household visits should continue
Comparison with Filtration- Chlorination Program in Rural Haiti • Technicians visit weekly • Sell chlorine • Provide replacement parts • Test chlorine residual • 1 tech : 200 households • Tech salary paid by US parish
What Has Been Demonstratedand Future Potential • With annual visits, high use (>75%) of consumable can be sustained over time • Potential exists to recover costs of visits and BCC through sales margin • Durable good must be sold below cost • Chlorine refills can be sold above cost with high use • Cost recovery is volume-dependent
Mesi anpil! Thank you! Acknowledgements • Dr. Gene Gangarosa, Emory • Dr. Bill Gallo, JSWF Project Director • Dr. Rochelle Rainey, USAID • Madame Eveline and JSWF staff
Jolivert Safe Water for Families Project Donate space and electricity Program Director, June 2008 Technical assistance & evaluation $20,000 grant from June 2006 - May 2008 Production and distribution of CDC’s Safe Water System
Pre-contemp-lation Contemp-lation Action Maintenance
KEY Summary construct PSI “Bubbles” determinant Stage of change Behavior change objective Opportunity Motivation Ability Availability / Transport costs Quality of care Social Norms Create aware- ness and trial Create repeat purchases Create trial Pre-contemp-lation: Non-member Contemp-lation: Non-purchaser Action: Inconsistent purchaser Maintenance: Consistent purchaser Attitudes Knowledge Social Support Outcome Expectations Ability to pay for bucket