Download
1 / 57
570 likes | 740 Views
Title from previous. Learning Objectives . Understand the formulary background, concept, structure , and ways formularies can facilitate better prescribing decision-making . Understand the concept of “ drugs of choice ”

E N D
Learning Objectives • Understand the formulary background, concept, structure, and ways formularies can facilitate better prescribing decision-making. • Understand the concept of “drugs of choice” • Critically discuss specific examples of local formulary decisions, and launch student projects for in-depth study of a formulary drug application case study. • Analyze controversies and issues surrounding formulary implementation and current practices
Outline - Hour 1 • Exercise: Formulary culture survey • Background & history of formularies • How formularies work • Examples from Cook County • Selective COX2 2. “Specific” criteria ?? • Global perspectives/examples • CDC Drugs of Choice 2. WHO Essential Drugs BREAK
Outline –Hour 2 • FLIP and formularies; FLIP tools • Audience Response Lab: Culture survey discussion • Project development • Assessment
Baghdad Basra
Baghdad Basra
Ancient Formulary Sumerian Cuneiform Tablet from Nippur 3000 BC
Early U.S. Formularies • Lititz Pharmacopoeia published in 1778 for use by the Continental forces • Coste’s Compendium Pharmaceuticum of 1780 used by French forces during the American Revolution • United States Pharmacopeia Convention meets in Old Senate Chamber Jan 1, 1820 • Selects drugs for the Pharmacopeia of the United States • Oldest non-profit organization in the U.S.
Drug Formulary: • “A continually updated list of medications and related information, representing the clinical judgment of physicians, pharmacists and other experts in the diagnosis and/or treatment of disease and promotion of health.” • Drug Formulary System: • Ongoing process • Collaboration of physicians, pharmacists, and other health care professionals • Establishes policies on the use of drug products and therapies most medically appropriate and cost-effective to best serve the health interests of a given patient population. • http://www.amcp.org/amcp.ark?c=stu&sc=glossary
Types of Formularies in U.S. Outpatient Public Sector Medicaid National VA (+ regional/local) Privatized-Public Sector Medicare Part D (2801 private plans) Private Sector PBMs Other HMO/Insurer Retail pharmacy chains Inpatient Hospital Formularies Nursing Homes
Formulary Management Drug Use Policy-making Drug Usage Monitoring Drug Use Drug Use Drug Use Drug Use Drug Use Drug Use Drug Use Pharmacy and Therapeutics Committee
Pharmacy and Therapeutics Committee Formulary Management Drug Use Policy-making Drug Usage Monitoring Drug Use Drug Use Drug Use Drug Use Drug Use Drug Use Drug Use
Pharmacy and Therapeutics Committee Formulary Management Drug Use Policy-making Drug Usage Monitoring • Additions • Deletions • Restrictions • Ensure Availability • Periodic Reviews • Publish Formulary • Communicate • Restrictions • Guidelines • Therapeutic Interchange • Lab Monitoring • Education • Alerts • Drug rep policies • Adverse Reactions • Med Error & Safety • Overall Utilization • Non-formulary Usage • Criteria-Based Monitoring
New Drug Requests by M.D.s Formulary Process Fill Out Application Formal Pharmacist’s Review Discuss at D&F Meeting Approved +/- Restrictions Approval by Exec Med Staff Not Approved Formulary Inclusion
Cook County COX2 Approval Mechanism (via Pharm HELP Desk) • GI Assessment Tool Scoring • Age (1-18) • Health Status (0-4) • RA (2) • Prednisone (5) • Ever GI Bleeding (8) • GI Side effects (2) Score • > 20 Automatic OK 16-20 Trial Salcylate
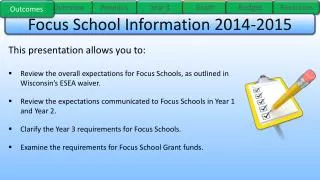
Trends in the Use of NSAIDs and Spending for Coxibs by Medicaid from 1999 through 2003 Fischer M et al. N Engl J Med 2004;351:2187-2194
COX2:NSAIDs %’s Cook County vs. Medicaid 2001 N=431/17,259
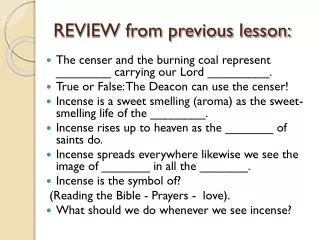
Percentage of Defined Daily Doses of NSAIDs Accounted for by Coxibs in the Fourth Quarter of 2003, According to Whether a Prior-Authorization Program Had Been Implemented Fischer M et al. N Engl J Med 2004;351:2187-2194
New Drug D & F Application 4 Roles of Specific Criteria • Organize evidence-based D&F review of value, indications, role for new drug • Educate, once drug approved • Guide real-time utilization of drug, ideally computer delivered at time of order • Retrospective review of appropriateness
Leading Challenges to CCH/UIC Formulary Committees • MD’s circumventing formulary and formulary application process for new drugs by using non-formulary ordering route • Inadequacies of the studies on which to base decisions • Lack of dedicated time of members to fully and critically digest literature and deliberate at the meetings • Wrestling with extremely costly ($10k/yr) new agents that appear to be effective, but pose major stain on institutions’ drug budget resources • Pharmaceutical industry influences and practices (including lobbying members, pricing schemes)
Methodology This report was produced through a multistage process. Beginning in 2004, CDC personnel and professionals knowledgeable in the field of STDs systematically reviewed evidence, including published abstracts and peer-reviewed journal articles concerning each of the major STDs, focusing on information that had become available since publication of the Sexually Transmitted Diseases Treatment Guidelines, 2002(1). Background papers were written and tables of evidence were constructed summarizing the type of study (e.g., randomized controlled trial or case series), study population and setting, treatments or other interventions, outcome measures assessed, reported findings, and weaknesses and biases in study design and analysis. A draft document was developed on the basis of the reviews. “CDC Drugs of Choice
WHO Essential Drugs List • In 1977, WHO published the first Model List of Essential Medicines containing 208 individual drugs which together could provide safe, effective treatment for the majority of communicable and non-communicable diseases
Bangladesh Essential Drugs Program-1982 • With these models, and inspired by WHO’s HFA program, in 1982 Bangladesh implemented its National Drug Policy (NDP). An expert committee assembled a list of recommendations based on WHO’s EDC, and the NDP aimed to ensure that procurement, local production, quality control, distribution, and use of pharmaceuticals came under the control of a single government body. This was to be a major part of national health policy.
No sooner had a form of the NDP been implemented than foreign-owned drug companies mobilized a campaign of misinformation, threats, and intimidation. For example, on June 1, 1982, the Bangladesh Times publicized the NDP. That same morning, the U.S. ambassador made an unscheduled call on the government to deliver the message that the policy was not acceptable to the U.S. government. Although the U.S. government had no overt interest in the NDP, drug companies, which had made considerable donations to the election campaigns of members of the U.S. government, assuredly did. They mobilized the influence their money had purchased against the NDP, which is why a superpower became involved in the internal health affairs of a small country on the other side of the globe
BreakDownstairs • Audience Response (30 minutes) • Formulary Myths • ISMP Data (“Myths are still true”) • Projects: Tools and drugs
Leveraging Formularies for Improved Prescribing • Venue for critical review of new drug claims • Evaluation of comparative efficacy • Less bias and conflict in decision-making • Cumulative expertise in reviewing new drugs • Experience with pitfalls and biases • Identify and weigh potentials for overuse/misuse • Weighing of cost benefit (for individual drug/indication) • Weigh institutional resource allocation (this drug vs. alternatives) • Raise/highlight safety concerns • Dissemination vehicles and tools (guidance and warnings) • More rational prescribing • Enhanced appropriateness and safety • Cost Effectiveness
Formulary Leveraged Curriculum Development & Dissemination Model Drug Info Specialists 12 ModulesPrinciples AdvancedSeminar Critical Knowledge Recommendations Drugs of Choice & Why Enhanced Input Restrictions/Guidelines for Appropriate Use Marketing Claims Formulary Decisionmaking Distillation of Drug Specific & Generic Issues Enhanced Output OtherLeaders Specialists Credibility Buy-in AttgMDs Residents Pharmacists Own Drug Delivery Use Criteria
Formulary Leveraged Curriculum Development & Dissemination Model Drug Info Specialists 14 ModulesPrinciples AdvancedSeminar Critical Knowledge Recommendations Drugs of Choice & Why Enhanced Input Restrictions/Guidelines for Appropriate Use Marketing Claims Formulary Decisionmaking Distillation of Drug Specific & Generic Issues Enhanced Output OtherLeaders Specialists Credibility Buy-in AttgMDs Residents Pharmcsts Own Drug Delivery Use Criteria
Causal empiricism FDA approval implies everyday use for all Interferes with clinical freedom Every patient is unique Specialist knows best Education requires experience with multiple drugs Widespread use = drug of choice Newer is better/safer Sicker patients need more drugs Formulary sacrifices patient care to cost Redundant with drug utilization review Formulary Myths Schiff, Rucker Med Care 1991
ISMP 2004 Survey Results Formulary Myths Still True !! • 70% reported causal empiricism comments impacting formulary decisions • 73% reported specialist knows best comments impacting formulary decisions • 49% reported never hearing FDA use implies everyday use for all comments in formulary deliberations http://www.ismp.org/Survey/surveyresults/Survey200411R.asp
MediMedia owns Triple I http://www.tripleimedimedia.com/about_us/