Download
1 / 29
290 likes | 449 Views

E N D
Pacific AIDS Education & Training Center2006 Southern California Forum on Rapid Testing Challenges & SolutionsI. Jean Davis, PhD, DC, PAAssistant Professor, Dept. Internal MedicineCharles R. Drew University of Medicine &Science University of California, Los AngelesCo- Principal Investigator & DirectorPacific AIDS Education & Training Centers National Minority AIDS Education & Training CentersMarch 23, 2006
Routine STD (HIV/Chlamydia/Gonorrhea) Counseling and Testing in the Urgent Care Unit of Martin Luther King / Charles Drew Medical Center Los Angeles County STD Program / Charles R. Drew University of Medicine and Science / Collaborative Alcohol Research Center Funded by National Center for HIV Prevention, CDC
Project Team Peter R. Kerndt, MD, MPH (LA-STD) Shahrzad H. Bazargan, PhD (Drew) Eric G. Bing, MD, PhD (Drew) Lisa V. Smith, MS, DrPH (LA-STD) Apurva Uniyal, MA (LA-STD) Marjan Javanbakht, PhD (LA-STD) Sheryl Lyss, MD (CDC, Project Officer)
Project Team Eugene Hardin, MD, (King-Drew) Wilbert Jordan, MD (Oasis Clinic) Chandra Higgins, MPH (LA-STD) Lina Sy, MPH (LA-STD) Guillermo Campos (LA-STD) Cynthia Davison (LA-STD) Jacqueline Moore (LA-STD)
Why should we use rapid tests in Urgent Care settings? • Recent advances in the treatment of HIV infection have increased the value of early diagnosis and medical intervention • Individuals identified with pre-clinical HIV infection can be referred for medical evaluation and treatment which improves the quality of life and survival of infected individuals • Since the approval of Oraquick HIV rapid test in 2002 and the rapid test’s categorization as a waived test under Clinical Laboratory Improvement Amendment in 2003, use of rapid HIV tests in clinical and non-clinical settings has increased dramatically
Goal • To assess the feasibility and acceptability of rapid HIV testing and STD screening in the Martin Luther King / Charles Drew Hospital Urgent Care Unit • To facilitate the transition from research protocol to programmatic screening and beyond
Why King-Drew? • King-Drew/SPA 6 • LA County’s highest chlamydia and gonorrhea rates • LA County’s3rd highest AIDS rates • Previous screenings suggest the true HIV prevalence lies between 0-10% • No systematic HIV/STD screening at the time of the study
Research & Programmatic Screening in KDMC Urgent Care: 10/03 to 11/05 1. Routine rapid HIV testing in the King-Drew Medical Center (KDMC) Urgent Care Unit Study: October 2003 – September 2004 2. Programmatic screening: October 2004 – November 2005
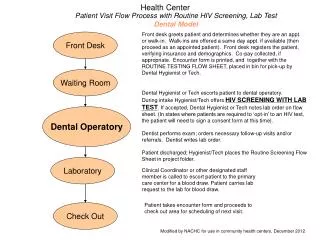
Patients admitted to Urgent Care Names listed on patient roster Screened for eligibility Ineligible (age, HIV+) Eligible HIV- , 18-54 y Not approached/ Not recommended Refused Accepted Rapid Study: Patient Recruitment
Patient Screening: Research Protocol Accepted Informed consent, Locator form, Data Collection form OraQuick Rapid HIV test (finger stick) Aptima 2 CHL & GC test (urine) Samples sent to Public Health Lab Negative Negative Client Satisfaction Survey Positive Positive Follow up by Public Health Investigators Confirm by Western Blot Refer to medical treatment and social services (OASIS)
Intake Forms & Client Satisfaction Survey • Intake Form: Patient’s age, race, gender, reason for refusing STD and/or HIV tests • Client Satisfaction Survey: 4-point Likert scale (1=strongly agree; 4=strongly disagree) 1. I understand the results of my test 2. I would recommend testing to a friend 3. I have tested in the past and I prefer receiving my results the same day 4. I found the rapid HIV test stressful 5. I received the results of my HIV test too quickly 6. I found the blood specimen draw uncomfortable 7. It would have been better to wait a week
HIV Testing with OraQuick Chlamydia and Gonorrhea Screening HIV CaseManagement Nutritional Counseling and Resources
Recruitment Summary: 10/03 – 9/05 2344 names abstracted from Urgent Care Roster 1342 Non-participants 1002 Participants* 98% age (<18 or >54) 2% HIV+ 120 Ineligible 576 Not approached Not in waiting room 2 Not recommended 50% mentally unstable 50% repeat visit 41% Recently tested 17% Too much pain/too sick 42% Other/Not specified 644 Refused *Participants also offered choice of testing for chlamydia and gonorrhea
Programmatic Screening Protocol10/04-11/05 Programmatic screening protocol similar to study protocol, which also included : • Intake Form: Patient’s age, race, and gender • Client Satisfaction Survey: 4-point Likert scale (1=strongly agree; 4=strongly disagree) With the exception of age, the patient’s demographics during programmatic screening were comparable to those obtained during the study protocol
Research & Programmatic Screening Summary: 10/03 to 11/05 • 2178 (63%) accepted HIV and/or STD screening tests: 55% Male 20% 18-29 years 22% 30-39 years 48% Black 48% Hispanic • 2139 (98%) tested with rapid HIV tests • 1543 (71%) tested with chlamydia/ gonorrhea tests
Research and programmatic screening detected numerous HIV/STD cases *Among HIV+; ** Among STD+, patients still being sought for treatment; Co-infections 3 chl/gc, 1 HIV/chl, and 1 HIV/gc
Client satisfaction with HIV rapid testing was very high during study protocol and programmatic screening sessions • 99% understood the results of their HIV test • 98% would recommend rapid testing to a friend • 93% of previous testers preferred same day test results* • 60% did not find the test stressful • 57% did not think they received HIV test result too quickly • 90% did not find the fingerstick uncomfortable • 93% did not feel it would have been better to wait a week for HIV test results n=2077; *n=1401; Satisfaction was comparable among HIV+ vs. HIV- patients
Patient / Staff Satisfaction “Thanks, man. I’ve been meaning to get this [HIV testing] done.” -Urgent Care Patient “Can my friends come and get tested?” -Urgent Care Patient “This is a good idea. Can you also screen in the parking lot in front of OASIS [clinic]?” -OASIS employee “We want everyone tested and flyers posted throughout the hospital. Testing should be a routine procedure.” -Urgent Care Nurse
Patient / Staff Satisfaction “Excellent project. It really helps the people who want to be tested , but can’t pay $80.00 for the Urgent Care/ER visit.” -Urgent Care Nurse “If you can’t screen everybody, make sure you screen the teenagers.” -Urgent Care Physician “This is great. Can you test my husband? I think he’s playin’ around.” -Urgent Care Patient
2nd degree burns to leg Calculus of the kidney Cellulitis Changing surgical dressing Chest pain/palpitations Conjunctivitis* Contusion of chest wall Dermatitis Diabetes Dizziness/giddiness Gastroenteritis Hair disease* Head & neck injury Headache Hypertension* Insect bite Lumbar sprain Neck sprain Objective tinnitus Sprain in lumbar region Upper respiratory infection Urinary tract infection* HIV/STD were detected among patients with non-HIV/STD discharge diagnoses *Discharge diagnoses for some HIV+ patients
Lessons Learned: KDMC • Rapid HIV testing is feasible at KDMC; high acceptance of Rapid HIV testing, despite very little advertising. • One of 100 KDMC Urgent Care patients tested positive for HIV and all HIV-positive patients received their test result (2,139 tested,1.2% HIV, 5.5% CHL/GC). • HIV prevalence was comparable with LAC STD clinics. Nearly half of the HIV infection was detected among the newly-infected patients.
Lessons Learned: KDMC • Close proximity of a case management program facilitated linkage to care; however, not all HIV+ patients accepted referral to services • Patient satisfaction with rapid HIV testing was high; KDMC staff satisfaction was equally high • KDMC has embraced rapid HIV testing, getting HIV test results in twenty minutes is warranted, and screening should be made available to patients of all ages, some in which HIV/STD would otherwise go undetected, through programmatic screening
Future Directions • Establish STAT laboratory to screen patients in the examination room • Explore implementation of “opt-out” program to increase the number of patients screened • In the meantime, increase advertising of the availability of HIV/STD in Urgent Care • Develop protocol to include rapid HIV test results into patients medical record
Contact Information Lisa V. Smith, MS DrPH Director, Epidemiology Unit Sexually Transmitted Disease Program 2615 South Grand Avenue, Room 500 Los Angeles, California 90007 Phone: 213-744-3120 Fax: 213-749-9606 lismith@ladhs.org