Download

1 / 19
300 likes | 1.78k Views
The Fascia Iliaca Compartment Block . 林必盛 中國醫藥大學 麻醉部. Indications.

E N D
The Fascia Iliaca Compartment Block 林必盛 中國醫藥大學 麻醉部
Indications • The Fascia Iliaca Compartment Block (FICB) is a simple block for post-operative pain relief for procedures and injuries involving the hip, anterior thigh, and knee. This block is useful, pre and post-operatively, for fractures of the hip and proximal femur, as well as total hip and knee arthroplasties.
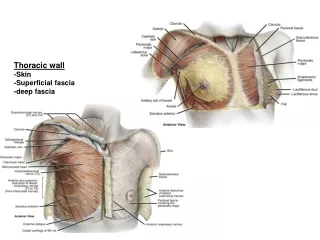
Lateral Femoral Cutaneous nerve • The Lateral Femoral Cutaneous nerve is a purely sensory nerve arising from the L2 & L3 nerve roots that provides sensation from the iliac crest down the lateral portion of the thigh to the area of the lateral femoral condyle. • The lateral femoral cutaneous nerve emerges from the lumbar plexus and travels downward lateral to the psoas muscle and crosses the iliacus muscle deep to the iliacus fascia.
Obturator nerves • The anterior and posterior Obturator nerves innervate a portion of the distal, medial thigh. They arise from the L2, L3, & L4 nerve roots and cross the iliacus muscle, deep to the fascia, to the medial thigh. The obturator nerves are sometimes involved in the FICB but probably plays little role in post-operative pain relief for most surgeries of the hip and proximal femur.
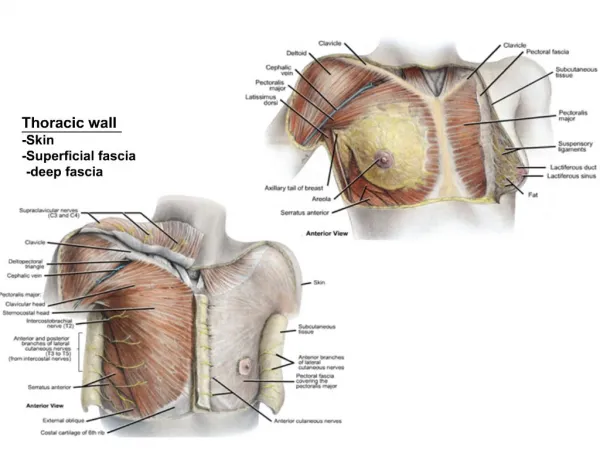
Iliacus muscle • The Iliacus muscle is a large, flat, triangular muscle that lines and fills the ilium. It originates from all along the upper portions of the ilium and iliac crest, sacrum and iliolumbar ligaments. The iliacus muscle joins with the lateral side of the psoas major muscle. Together they are referred to as the iliopsoas. The iliopsoas exits the pelvis from beneath the inguinal ligament, wraps around the proximal neck, and inserts into the lesser trochanter, acting as a powerful hip flexor.
Fascia Iliaca • The fascial covering of the iliopsoas is thin superiorly, becoming significantly thicker as it reaches the level of the inguinal ligament. This thickness provides a great deal of resistance and a large “pop” as a needle tip is passed through the fascia.
Lumbar plexus • The lumbar plexus is made up of the nerve roots from the T12 through L5 vertebrae. The largest branch of the lumbar plexus is the Femoral nerve is, arising from the L2, L3, & L4 roots. The femoral nerve descends through the fibers of the psoas major and exits at the lower portion of the psoas' lateral border, passing downward between the psoas and iliacus muscle, deep to the iliacus fascia. The femoral nerve exits the pelvis into the upper thigh, lateral to the common femoral artery and vein.
Conventional Fascia Iliaca block • This block use only surface landmarks and the feel of the needle as it passes the fascia lata and the iliacus fascia (2 pops), to position the needle. • Introduce a needle just beneath that fascia. • Local anesthetic solution is then injected, creating a local anesthetic filled space below the fascia. • As this local-filled space increases in size during injection, the fluid travels cephalad beneath the fascia and contacts the nerves of the lumbar plexus which are located there. • These nerves are the lateral femoral cutaneous nerve, the femoral nerve and the obturator nerves.
FICB block performed with the ultrasound • Uses ultrasound to locate the superficial fascial layer of the iliopsoas muscle at the anterior edge of the ilium. • Ultrasound can assure that the needle tip is not only in the correct plane, but to allow the operator to safely advance the needle further into the fluid filled space after the initial bolus of local anesthetic solution is concluded. • Ultrasound also allow the operator to directly observe the spread of the local solution cephalad, towards the superior ilium during injection.
Practical points • Since this is a compartment block, it needs use a fairly large amount of volume to assure adequate spread of the solution in the compartment, 40 to 50 mls being commonly used. • As a routine, use a total of 50 ml of local anesthetic mixture injected incrementally, 10 – 15 ml after needle placement. • Advance the needle into the space created by the volume, then inject the remainder of the local anesthetic mix.
Alternate methods • Some centers advocate injecting a bolus of normal saline after the initial needle placement, to initiate hydro-dissection of the sub-fascial plane, followed by the local anesthetic solution. • While this technique seems reasonable, since the saline and the local will eventually occupy the same space, it makes more sense to simply start and end with the solution of the final concentration.
Important notes • Aspirate occasionally during injection of the local. • When performing the fascia iliaca block you will generally not see the local solution accumulating at the site of injection. More commonly the local solution will spread along the planes almost as soon as it is injected. • If you feel excessive resistance to injection, either withdraw the needle slightly or advance it, • Place manual pressure inferior to the injection site to encourage antegrade flow towards the lumbar plexus.
CATHETER INSERTIONS • If you are inserting a catheter into the fascia iliaca compartment, do so after you have injected all of the solutions. This will make sure there is ample space for the catheter to move into as it is inserted. • Too long a catheter may have a risk to migrate out of the compartment. • I.V. catheter may get kinked with the posture of the patient and a stent inside the catheter can prevent such condition.
Resident training • 3 residents: 1 R2 and 2 R3. • Each has at least 3 hand on experiences. • After which validation of correct placement was made with ultrasound.