Download
1 / 36
360 likes | 368 Views
Learn to localize lesions in the nervous system and differentiate between vascular and demyelinating or neoplastic presentations of brainstem lesions. Case studies included.

E N D
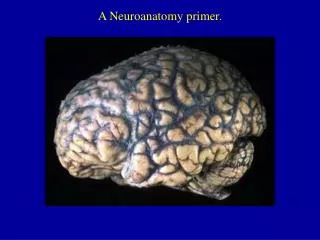
Neuroanatomy Meds IV Shannon L Venance, MD PhD
Objectives: • At the end of this session, provided with a history and exam, participants will be able: • Localize the lesion to the appropriate part of the nervous system • Compare and contrast vascular with demyelinating or neoplastic presentations of brainstem lesions.
Case 1 • A 47 year old man presents with a decreased level of consciousness (LOC). • He complained of an sudden posterior occipital headache with R face tingling and drooping and then collapsed to knees(1130 hrs) while remaining alert. • On route to hospital, seizure activity noted and he was intubated on arrival to the community ER and loaded with dilantin. • He was transferred to Victoria Hospital as there were no ICU beds available locally.
Case 1 continued….. • PMHx: brief episodes of vertigo, dysarthria, collapsing (seconds to minutes only) for 8 months; otherwise healthy • Med: ASA • NKDA • Soc Hx: married with 3 children
Case 1 24 hrs after presentation • hemodynamically stable • intubated and fully ventilated, no sedating drugs • unresponsive to voice • no spontaneous eye opening • pupils were pinpoint and reactive • no horizontal eye movements with oculocephalic maneuver (OCM) • absent corneal reflexes, no response to nasal tickle • weak gag, constant hiccoughing ~ 1-2/min • tone was reduced with brisk withdrawal to noxious stimuli in the legs bilaterally • reflexes present, left > right; toes ↓↓
patient normal
Case 1 48 hrs after presentation • intubated, no breathing over the vent • pupils were fixed and dilated • no eye movements with OCM • corneals and nasal tickle absent • no gag, no hiccoughs • flaccid tone • no response to noxious stimuli all 4 extremities • reflexes left > right; toes ↑↑
http://www.med-ed.virginia.edu/courses/rad/headct/index.html
Case 2 • 32 yo male presents with a 6 month history of intermittent bifrontal headache with progressive symptoms • 3 months of intermittent diplopia on looking right or left (no improvement with prism glasses) • headache became constant, associated with mild nausea, worse in the mornings • 2 months of right side weakness and incoordination (dropping glasses, r leg buckling, falling to the right) • 1 month right facial numbness • choking on liquids and had nasal regurgitation with coffee, tea • symptoms worsened 1 week prior with a viral illness and fever
Case 2 • normal mental status • pupils 8 mm OS and 6 mm OD, reactive, no APD • restriction of right eye abduction with nystagmus • vertical nystagmus on upgaze • reduced pinprick right V1, V2, V3 • right lower motor neuron type facial palsy • palate deviated to the right, tongue midline • flaccid, hypophonic dysarthria • right arm/leg spasticity with ankle clonus • R>L hyperreflexia with extensor plantar response bilaterally • mild pyramidal weakness on the R • dysmetria right > left
“control” patient
Case 3 • Francois, a 48 yo right handed man woke this morning with weakness involving the entire left side of his face. • Two days prior he noticed pain behind the left ear which continues. His breakfast tasted “strange” this morning. He has no other symptoms and he has otherwise been well. • Your focused exam reveals normal tympanic membranes, full extraocular movements, a left lower motor neuron facial weakness (reduced forehead wrinkling, eye closure and grimace) with a midline tongue and palate. He hears sounds more loudly in his left ear. No pronator drift. Deep tendon reflexes are 2+ symmetrical with flexor plantar responses.
Which of the following statements about facial weakness is true? • Ramsay-Hunt syndrome is a cranial nerve VII palsy associated with lateral rectus paralysis. • Prednisone is the treatment of choice for Bell’s palsy when started within 48 hours of onset. • Lower motor neuron facial palsy involves paresis/paralysis of the lower facial quadrant only. • There is no risk of recurrence with a Bell’s palsy. • Cranial nerve nuclei located in the pons along with the facial nucleus include CN III, IV and VI
Case 4 • 53 yo woman develops sudden onset of left sided weakness, right facial weakness and double vision 2 weeks after an MI treated with angioplasty • PMHx also includes hypertension, stopped smoking 2 weeks ago (prev 25 ppy hx) • her medications include ASA, ramipril, metoprolol and lipitor
Case 4 • abnormal eye movements on looking left • right eye does not adduct but convergence is spared (right eye adducts and pupil constricts) • left eye abducts with left-beating nystagmus • vertical eye movements are normal • weakness of the right face including the forehead • weakness of the left arm and leg ~4/5 in a pyramidal distribution • reflexes, L brisker than R with an upgoing L toe
http://upload.wikimedia.org/wikipedia/en/thumb/b/b0/Internuclear_ophthalmoplegia.jpg/180px-Internuclear_ophthalmoplegia.jpghttp://upload.wikimedia.org/wikipedia/en/thumb/b/b0/Internuclear_ophthalmoplegia.jpg/180px-Internuclear_ophthalmoplegia.jpg
82 year old had been followed for many years, on levodopa/carbidopa for a degenerative process causing a rest tremor, slowness and stiffness of movement, soft voice with drooling and dysphagia; he had been falling more recently • died of complications after sustaining a hip fracture from a fall
Case • 55 yo emaciated and dishevelled woman was found wandering on the streets and brought to the ER on Christmas Day • she knew her name but was not oriented to date or time and could not give her age or address but provided a rich story which could not be corroborated • language was normal but she was unable to recall 3 items after 2 minutes; 5 minutes later she denied having seen you before; otherwise reading, writing and higher mental functions were normal • her neurologic exam was otherwise normal • while waiting for the neurology resident, she was given a tray of holiday goodies which she devoured • No known medical history, medications, allergies
on examination 2 hours later, she was slightly drowsy but rousable, not oriented to month or year and thought the resident was her boyfriend • she had nystagmus in all directions of gaze and her gaze was dysconjugate when looking right or left • normal strength, reflexes 2+ except ankles 1+ and her toes were upgoing bilaterally • mild reduction in vibration at the toes • she was unable to heel-shin bilaterally and her gait is wide-based and markedly ataxic
http://medlib.med.utah.edu/WebPath/CNSHTML/CNS083.html http://www.urmc.rochester.edu/neuroslides/slide157.html
Summary: clinical brainstem • CN III – XII symptoms and signs • crossed sensory or motor findings • coordination, ocular, vertigo acute onset • abrupt is vascular; if over hours – toxic, metabolic • if LOC, remember reticular activating system (RAS) within brainstem is responsible for alertness • chronic • over weeks to months; neoplastic, demyelinating, degenerative
http://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpghttp://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpg
http://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpghttp://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpg
http://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpghttp://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpg
http://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpghttp://www.meddean.luc.edu/lumen/MedEd/Images/NeuroLab/nl35sl.jpg