Download
1 / 35
370 likes | 890 Views
Rupture AAA – Any NEW advances?. Dr Karen Tung Lok Man PYNEH. Epidemiology in HK. ~ 900 new cases AAA diagnosed every year 10% presented as rupture Operative mortality rate : Elective 10% Rupture 54%. Stephen W.K. Cheng World J. Surg 2003. Rupture AAA.

E N D
Rupture AAA – Any NEW advances? Dr Karen Tung Lok Man PYNEH
Epidemiology in HK • ~ 900 new cases AAA diagnosed every year • 10% presented as rupture • Operative mortality rate : • Elective 10% • Rupture 54% Stephen W.K. Cheng World J. Surg 2003
Rupture AAA • 50% die before reaching hospital • 30% who reached hospital die before operation • Operative mortality : 50% Overall mortality rate : 80 -90%
Open AAA repair • 30 days operative mortality rate : • 48% in 1998 41% in 2001 Are we satisfied with this improvement ? M.J. Bown British Journal of Surgery 2002
Title • Lorem ipsum dolor sit amet, consectetuer adipiscing elit. Vivamus et magna. Fusce sed sem sed magna suscipit egestas. • Lorem ipsum dolor sit amet, consectetuer adipiscing elit. Vivamus et magna. Fusce sed sem sed magna suscipit egestas. Room for improvement ?
Endovascular AAA repair (EVAR) • EVAR was first performed in human by Dr Juan Parodi in 1991
Benefits of EVAR on elective AAA 30 days mortality rate Long term aneurysm-related death ICU stay and total hospital stay R M Greenhalgh Lancet 2005 Jan D. Blankensteijin New Eng J Med 2005 R. E. Lovegrove British Journal of Surgery 2008
EVAR in rupture AAA ? • 1st EVAR was performed in 1994 on a 61-year-old man with 6cm rupture AAA • Duplex scan on day 6 : no leakage • Discharged on day 7 S W Yusuf The Lancet 1994
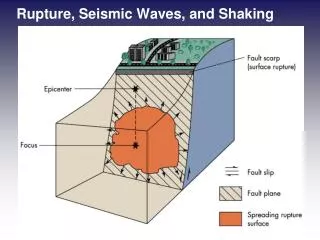
Technique of emergency EVAR • LA common femoral artery cutdown • Placement of large sheath • Aortic occlusion balloon is inserted in supra-renal position Manish Mehta J Vasc Surg 2010
Technique of emergency EVAR • GA • Stent graft main body is inserted on the contra-lateral side • Arteriogram is done on ipslateral side with aortic balloon temporaily deflated • Stent graft main body is rapidly deployed Manish Mehta J Vasc Surg 2010
Technique of emergency EVAR • Aortic balloon advances back and inflats below renal artery • Contra-lateral limb extension is deployed • Aortic balloon is removed • Ipsilateral limb extension is deployed Manish Mehta J Vasc Surg 2010
Anatomic suitability for elective EVAR >=15mm < 30mm < 60o >=7mm
Anatomic suitability for rAAA EVAR Dieter Mayer Annuals of Surgery 2009 Loosen Anatomic criteria Randy Moore J Vasc Surg 2007
Current AAA management Permissive Hypotension : NO fluid resuscitation unless SBP < 80mmHg or mentation K.Roberts Eur J Vas 2006 N Rupture AAA Stable Open repair Y SBP >80 mmHg & Normal mentation Permissive Hypotension N Spiral CTA Endo Candidate EVAR Y
Retrospective studies • 90 rupture AAA patients with EVAR done in 7 years • 30 days mortality : 27% J.Hoist Eur J Vasc Endovasc Surg 2009 • 102 rupture AAA patients with EVAR done in 10 years • 30 days mortality : 13% Dieter Mayer Annuals of Surgery 2009
New Hope EVAR is a valid treatment option for rAAAwhen used as a first-line method for all patients
Systematic review • 1 RCT and 33 non-randomised case series (24 retrospective and 9 prospective) reports were identifed D.W. Harkin Eur J Vasc Endovasc Surg 2007
Systematic review Mortality ( EVAR : 17% , Open : 34%) D.W. Harkin Eur J Vasc Endovasc Surg 2007
Selection Bias • EVAR groups were more stable than open groups • EVAR groups had technically easier anatomy (e.g. longer aortic neck) • CT delayed treatment for open AAA repair
1st RCT EVAR Vs Open repair • Sept 2002 – Dec 2004 • Single centre prospective randomized controlled trial R.J. Hinchliffe Eur J Vasc Endovasc Surg 2006
1st RCT EVAR Vs Open repair Failed to demonstrate superiority of EVAR over open repair
Advantages of emergency EVAR • Avoid vasodilating and negatively inotropic effects of GA • Avoid large midline laparotomy on muscle wall tone which lead to circulatory compromise • Decreased surgical dissection blood loss • Avoid aortic cross-clamping and potential reperfusion injury
Limitations of EVAR in rupture AAA • Anatomical issue • Logistical issue – Lack of availability of EVAR trained staff and appropiate endograft components • EVAR specific complications need re-intervention
Is EVAR superior to open repair for rupture AAA ? Can we improve outcome of rupture AAA patients by incorporating EVAR into our protocol?
Rupture AAA protocol AIM : To demonstrate any improved survival (30 days mortality) after introduction of an rupture AAA protocol 2001 2004 2006 Randy Moore J Vasc Surg 2007
Result Randy Moore J Vasc Surg 2007
Result Randy Moore J Vasc Surg 2007
Conclusion • Mortality rate for open repair of rupture AAA remains high • Emergency EVAR for treatment of rupture AAA is feasible • Introduction of rupture AAA repair protocol includes EVAR can improve mortality rate
What is going on... 3 Randomized controll trials currently undergoing The Amsterdam Acute Endovascular Treatment To Imporve Outcome of Rupture Aorta-Iliac Aneuysm trial (AJAX) The Rupture Aorta-Iliac Aneuysm Endo vs Surgery (ECAR) trial Immediate Management of the Patient with Rupture: Open Versus Endovascular Repair (IMPROVE) trial