Download
1 / 1
10 likes | 85 Views
Severity assessment for lower respiratory tract infections: potential use and validity of CRB-65 in primary care N. Francis, J. Cals , C. Butler, K. Hood, T. Verheij , P. Little, H. Goossens , S. Coenen , on behalf of the GRACE Project Group. Introduction and purpose

E N D
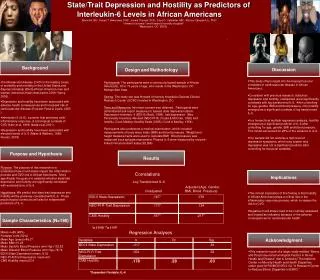
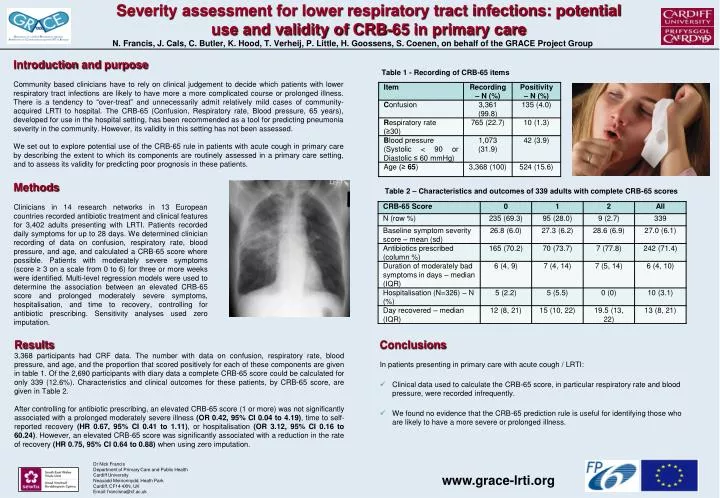
Severity assessment for lower respiratory tract infections: potential use and validity of CRB-65 in primary care N. Francis, J. Cals, C. Butler, K. Hood, T. Verheij, P. Little, H. Goossens, S. Coenen, on behalf of the GRACE Project Group Introduction and purpose Community based clinicians have to rely on clinical judgement to decide which patients with lower respiratory tract infections are likely to have more a more complicated course or prolonged illness. There is a tendency to “over-treat” and unnecessarily admit relatively mild cases of community-acquired LRTI to hospital. The CRB-65 (Confusion, Respiratory rate, Blood pressure, 65 years), developed for use in the hospital setting, has been recommended as a tool for predicting pneumonia severity in the community. However, its validity in this setting has not been assessed. We set out to explore potential use of the CRB-65 rule in patients with acute cough in primary care by describing the extent to which its components are routinely assessed in a primary care setting, and to assess its validity for predicting poor prognosis in these patients. Table 1 - Recording of CRB-65 items Methods Clinicians in 14 research networks in 13 European countries recorded antibiotic treatment and clinical features for 3,402 adults presenting with LRTI. Patients recorded daily symptoms for up to 28 days. We determined clinician recording of data on confusion, respiratory rate, blood pressure, and age, and calculated a CRB-65 score where possible. Patients with moderately severe symptoms (score ≥ 3 on a scale from 0 to 6) for three or more weeks were identified. Multi-level regression models were used to determine the association between an elevated CRB-65 score and prolonged moderately severe symptoms, hospitalisation, and time to recovery, controlling for antibiotic prescribing. Sensitivity analyses used zero imputation. Table 2 – Characteristics and outcomes of 339 adults with complete CRB-65 scores Results 3,368 participants had CRF data. The number with data on confusion, respiratory rate, blood pressure, and age, and the proportion that scored positively for each of these components are given in table 1. Of the 2,690 participants with diary data a complete CRB-65 score could be calculated for only 339 (12.6%). Characteristics and clinical outcomes for these patients, by CRB-65 score, are given in Table 2. After controlling for antibiotic prescribing, an elevated CRB-65 score (1 or more) was not significantly associated with a prolonged moderately severe illness (OR 0.42, 95% CI 0.04 to 4.19), time to self-reported recovery (HR 0.67, 95% CI 0.41 to 1.11), or hospitalisation (OR 3.12, 95% CI 0.16 to 60.24). However, an elevated CRB-65 score was significantly associated with a reduction in the rate of recovery (HR 0.75, 95% CI 0.64 to 0.88) when using zero imputation. Conclusions In patients presenting in primary care with acute cough / LRTI: • Clinical data used to calculate the CRB-65 score, in particular respiratory rate and blood pressure, were recorded infrequently. • We found no evidence that the CRB-65 prediction rule is useful for identifying those who are likely to have a more severe or prolonged illness. Dr Nick Francis Department of Primary Care and Public Health Cardiff University Neauadd Meirionnydd, Heath Park Cardiff, CF14 4XN, UK Email: francisna@cf.ac.uk www.grace-lrti.org