Download
1 / 22
230 likes | 397 Views
Case Studies on Insulin Initiation. Nicole McGrath 2013. Case 1. 52 year old woman, type 2 diabetes for 10 yrs, BMI 32 (87kg) On Metformin 850mg mane, 1700mg nocte; Gliclazide 80mg bd Regularly picks up scripts; assures you she is taking Not testing BG HbA1c 70 mmol /mol

E N D
Case Studies on Insulin Initiation Nicole McGrath 2013
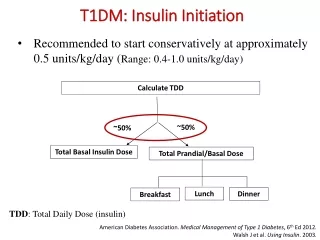
Case 1 • 52 year old woman, type 2 diabetes for 10 yrs, BMI 32 (87kg) • On Metformin 850mg mane, 1700mg nocte; Gliclazide 80mg bd • Regularly picks up scripts; assures you she is taking • Not testing BG • HbA1c 70 mmol/mol • What to do?
Case 1 Discussion • Increase Gliclazide to 160mg bd • Start home BG testing • BG elevated: • Fasting around 10 • Before evening meal 12 • 2 hours after evening meal 13 • What next?
Case Study 1 - Mrs JAge 52. BMI 32 (87kg). HbA1c: 70mmol/mol Currently on: Metformin 850mg mane, 1,700mg at dinner, Gliclazide 160mg BD. Blood glucose (mmol/L) How would you start Mrs J. on insulin?
Case Study 1 - Mrs J. • NZGG: • Start Isophane 8-10 units at bedtime. • Continue orals – consider reduction of Gliclazide to 80mg BD. • Give the patient instruction to self-adjust insulin dose. • Likely doses to achieve red line: • Isophane 30-35 units nocte • Gliclazide 160mg bd • Metformin 850mg mane, 1700mg evening meal
Case Study 2 – Mrs T:Age 74. HbA1c 75mmol/mol (9%) , Currently on: Prednisone 5mg/day for Rheumatoid Arthritis and maximal OHA therapy. Blood glucose (mmol/L)
Case Study 2 – Mrs T. As you can see… high glucose levels rising during the day but dropping over night. Consider: • 10 units of isophane at breakfast and adjust the dose as required. • Good fasting achieved with 15 units but…. Red line still suboptimal so change to • 15 units of Pre-mixed insulin breakfast • Penmix 30 / Humulin 30/70 .
Case 3: 66 yr old male with COPD • On Metformin 1gm bd, Glipizide 5mg bd; • HbA1c 57 mmol/mol • Needs course of Prednisone for exacerbation COPD • Prednisone 40mg daily 5 days then 20mg 5 days
PATHWAY FOR MANAGING HYPERGLYCAEMIA SECONDARY TO STEROIDS FOR CLIENTS WITH COPD(on HealthPoint) • Whilst on 40 mg Prednisone • Test BSLs at least tds • OHAs –increase usual mane dose by 100% e.g. usual mane dose Gliclazide 80mg –increase to 160mg • If patient is maximised on OHAs: • transient hyperglycemia can sometimes be tolerated for a short period. • Alternatively, a morning dose of Penmix 30/70 (usually 0.2 units/kg body weight) can be given during steroid treatment. • Some patients may need to be commenced on ongoing insulin
Case Study 4 - Mr L. Age 62. BMI 27 (78kg) HbA1c 68mmol/mol. Currently on: maximal OHA therapy. Blood glucose (mmol/L)
Case Study 4 – Mr L. High fasting and post-prandial BG: basal insulin with current OHA will treat fasting hyperglycaemia but not post meal BG elevations Suggest Premixed insulin: As lunch not so much of an issue, Novomix 30 or Humalog 25: Start 15 units bd (0.2 units/kg/dose) Stop sulphonylurea
Case Study 5 - Mr K. Age 64. HbA1c 75mmol/mol (9%). Currently on: maximal OHA therapy. Blood glucose (mmol/L)
Case Study 5 – Mr K. MrK’s blood glucose is particularly high after his main meal (dinner). • Consider 10–12 units of pre-mixed insulin (Humalog Mix25 or Novomix30) at dinner.
Case 6: 55 yr old male, BMI 35 (116kg), known diabetes 4 yrs, Hba1c 85 • No home BG testing • Long gaps between prescription requests • Prescribed Metformin 1gm bd, Gliclazide 160mg bd • Microalbuminuria, background retinopathy, hypertension
Case 6 • Option 1 • advice on diet, exercise, taking medication • warn of possible adverse consequences; • increase Metformin to 1500mg bd; • Start BG testing and reporting back to nurse
Case 6 • Option 2: 3 month F/U HbA1c 76: • Has achieved good reduction with compliance but HbA1c still suboptimal and not testing much • Fasting BG 10, Pre-dinner 13 • Glargine in addition to Metformin and Gliclazide a reasonable option • Starting dose: 0.2 units / kg / day: • Weight 116kg: start 24 units daily (morning or night) • Insulin self-adjustment in conjunction with weekly contact with nurse
Case 6 • Option 3: • Accept failure of OHA • Prescribe pre-mixed insulin bd • He eats 2 meals per day: brunch and dinner • NovoMix 30 or Humalog Mix 25: 24 units bd • Could well need to double that • Stop sulphonylurea, continue Metformin • Provide insulin self-adjustment handout or ask pt to increase each dose by 2 units every 3 days until BG 4-8 • Hopefully practice nurse will be able to contact him weekly to support/supervise
Case 7: 37 year old female, BMI 45 (weight 128kg); diabetes 3 years • HbA1c 85 • Prescribed Metformin 1gm bd; Gliclazide 160mg bd and appears to be taking them • Not testing BG • Sleep Apnoea
Case 7 • Option 1 • Weight loss essential: • Refer to dietitian for consideration of Optifast • Refer for consideration Bariatric Surgery • Pioglitazone in addition to Metformin and Gliclazide • Repeat HbA1c in 3 months
Case 7 • Option 2 • Accept weight loss/exercise not achievable • Consider insulin, although insulin resistance will mean large doses necessary • Eats 3 meals per day and snacks in the evening • Penmix 30 or Humulin 30/70: 26 units bd, stop sulphonylurea • Insulin self-adjustment: may need to increase by > 4 units each time if BG remain very high • Will probably need 60 units bd if she doesn’t change her diet/weight
Case 8: 41 yr old male, BMI 27 • Diabetes 8 yrs, on Metformin 1500mg bd, Gliclazide 160mg bd, Pioglitazone 45mg daily • Truck driver • HbA1c 62 mmol/mol • Microalbuminuria, erectile dysfunction, retinopathy • BG: fasting 9, pre-dinner 10 • Requires heavy traffic licence medical certificate • Patient feels he is doing as much as he can re diet, exercise
Case 8 • Needs insulin but want to minimise effect on driving • Isophane at night 10 units • Increase by 2-4 units every 3 days to achieve fasting BG < 7 • Continue OHA • NB. LTSA do not generally require specialist reports for type 2 patients on insulin