Download
1 / 18
250 likes | 564 Views
Insulin Initiation In Primary Care. Dr Arla Ogilvie Endocrinologist Watford General Hospital West Herts Hospitals NHS Trust. Does the Patient Need Insulin?. ?Is it appropriate for the patient to be managed in Primary Care? ?Sufficient Knowledge Skills Support Time Confidence

E N D
Insulin Initiation In Primary Care Dr Arla Ogilvie Endocrinologist Watford General Hospital West Herts Hospitals NHS Trust
Does the Patient Need Insulin? ?Is it appropriate for the patient to be managed in Primary Care? ?Sufficient Knowledge Skills Support Time Confidence ? Have all other factors relating to control been addressed
Liver Muscle Insulin Resistance….3Types Patient Metabolic Doctor
Understand the patient Is insulin necessary? Factors in poor control Diet and ex Compliance with Rx Health beliefs Fears Hypoglycaemia Weight gain Occupation Understand the insulin Type and regime Once daily + oral agents Twice daily premix (Basal bolus???) Starting dose Patient EDUCATION TIME for follow up Dose titration Regular review and support Before you start……
Setting Individual Goals • Optimise blood glucose control • Keep patient asymptomatic • Prevent long term complications • Avoid hypoglycaemia • Preserve Quality of Life Safety is paramount!
Self-monitoring of blood glucose • Monitoring glucose is essential for safe and successful insulin treatment: • It guides dose adjustment • It allows patients to see the impact of behaviours and diet on glucose • Patients MUST know how to monitor glucose • The most important aspect of self-monitoring is that the patients DO something with the results Diabetes UK. http://www.diabetes.org.uk/hcpreports/primary_recs.pdf, 2005 National Diabetes Support Team. http://www.cgsupport.nhs.uk/downloads/NDST/Factsheet_Glucose_Self_Monitoring.pdf, 2005NICE. http://www.nice.org.uk/page.aspx?o=36882, 2005. Owens D et al. Diabetes and Primary Care 2004;6:8–16
Once-daily basal insulin • Duration depends on the insulin • Insulin analogues may provide 24-hour cover • Intermediate isophane preparations (Insulatard and Humulin I) may only be active for 8 – 18 hours and have a more pronounced peak activity Insulin activity Time (8–24 hours) Insulin Schematic representation
Benefits of a once-daily basal insulin regimen • One injection per day • Useful for patients reluctant to start insulin treatment • Works best for morning hyperglycaemia • Useful where someone else has to administer insulin • May help overcome fear of starting insulin • Some basal insulin injections may provide a weight benefit1 1.Philis-Tsimikas A et al. Clin Ther 2006;28:1569–81
Limitations of once-daily basal insulin regimen • Does not provide insulin for post-meal glucose surges: • Assumes patient can produce sufficient insulin to cover these mealtime requirements • Requires a fairly strict, predictable diet: • Dosing during the day is inflexible and so patients need to intake similar calories each day
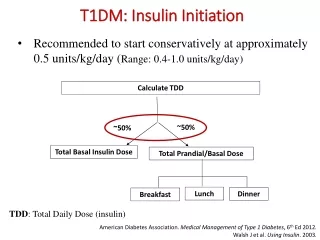
TYPE 2 Nocte Isophane insulin Insulatard or Humulin I Start 10units + Metfomin and Sulphonylurea (Glitazone) Titrate once or twice weekly How Much? • Newer agents • Gliptins • GLP1 Analogues • Are NOT licensed • To be given with • insulin
Easy Dose Adjustment for Once Daily Basal Insulin • The 3 – 0 – 3 Rule • After Initiation • Adjust insulin every 3 days • Based on fasting glucose • If average glu > 7 – increase by 3 units • If glu < 4mmol/l decrease by 3 units
Premixed insulin • Basal + Rapid acting component • Possible regimens: • Once daily with largest daily meal (usually dinner) • Twice daily with dinner and breakfast • Three times daily, with each meal Insulin activity Brkfast Lunch Dinner Bedtime Mixtard 30 – may need snacks Wait 30 mins between injecting and eating Novomix 30 No snacks needed Inject and eat immediately
Benefits of a premixed insulin regimen • Targets mealtime glucose • Can be initiated as one injection per day to familiarise patient with injecting (Most need twice daily) • Second or third injections of same insulin can be added if necessary to optimise control • Need fairly regular lifestyles, Eat similar amounts at similar times 1. Garber AJ et al. Diabetes Obes Metab 2006;8:58–66
Analogue basal-bolus therapy Rapid insulin Rapid insulin Rapid insulin Rapid-acting insulin Long-acting insulin Long-acting insulin Insulin activity Breakfast Lunch Dinner Bedtime
Benefits of a basal-bolus insulin regimen • Closest to natural insulin production by the body • Not necessary for majority of Type 2 • May be needed for those who have erratic mealtimes, work variable shifts • Gives more flexibility over type of food and when it can be eaten • Suited to those who are highly motivated • Need to monitor 4 times daily to optimise doses
Insulin with or without oral agents? • Oral agents can be continued when once daily basal insulin is initiated • It is recommended that metformin is continued where possible in T2 DM • Stop Sulphonylurea with premixed insulin • Glitazones can be used with insulin – usually where intolerant to metformin. Oedema may be a problem
Commencing Insulin Therapy • Ensure patient can blood glucose monitor and understands BG targets • Assess patient for suitable device • Educate patient regarding : • Storage, timing and action of insulin. • Device use and safety • Injection technique, sites and rotation. • Hypoglycaemia • Driving safety and legal Implications • Sick day Rules – • Dose Adjustment and exercise ( if suitable) • After education full assessment carried out to ensure patient competence and safety.
POOR CONTROL -Troubleshooting! • Compliance - Rx, lifestyle, acceptance • Unable to use Pen - check technique • Withdrawing needle too soon - ‘count to 10’ • Site problems -random rotation/hypertrophy • Wrong timing of injections • Eating to avoid hypos • Rebound hyperglycaemia- check Sx of hypo