Download
1 / 41
480 likes | 633 Views
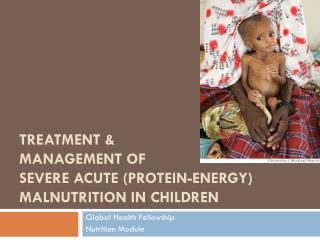
Chapter 7 Severe acute malnutrition. Case study: Kobi. Kobi , a 12-month-old boy brought to district hospital from a rural area . Kobi had an 8 day history of loose watery stools. 2 days of increased irritability and poor oral intake.

E N D
Case study: Kobi Kobi, a 12-month-old boy brought to district hospital from a rural area. Kobi had an 8 day history of loose watery stools. 2 days of increased irritability and poor oral intake.
Stages in the management of a sick child(Ref. Chart 1, p. xxii) • Triage • Emergency treatment • History and examination • Laboratory investigations, if required • Main diagnosis and other diagnoses • Treatment • Supportive care • Monitoring • Plan discharge • Follow-up
What emergency and priority signs does Kobi have Temperature: 34.8o CRR 50, pulse 130/min, Pulse volume normal Weight: 6.0 kgLength: 69 cm Capillary return <3 seconds SpO2 92%
Triage Emergency signs (Ref. p. 2, 6) • Obstructed breathing • Severe respiratory distress • Central cyanosis • Signs of shock • Coma • Convulsions • Severe dehydration Priority signs (Ref. p. 6) • Tiny baby • Temperature • Trauma • Pallor • Poisoning • Pain (severe) • Respiratory distress • Restless, irritable, lethargic • Referral • Malnutrition • Oedema of both feet • Burns
Triage Emergency signs (Ref. p. 2, 6) • Obstructed breathing • Severe respiratory distress • Central cyanosis • Signs of shock • Coma • Convulsions • Severe dehydration Priority signs (Ref. p. 6) • Tiny baby • Temperature • Trauma • Pallor • Poisoning • Pain (severe) • Respiratory distress • Restless, irritable, lethargic • Referral • Malnutrition • Oedema of both feet • Burns
History Kobi was well until 5 months of age. At 5 months his mother became pregnant again. His mother had started to wean him from the breast at 3 months, as her milk supply was reduced. From 4 months he was fed formula milk from a bottle with a rubber teat. He was given solid food from four months of age, mostly potatoes and some vegetables. From 5 months he had six episodes of diarrhoea. Each lasted 5-6 days. During each episode of diarrhoea he was given reduced amounts of fluid and feeds because his mother thought this would reduce the severity of his diarrhoea. On this last occasion he was taken to the hospital, as he became irritable and was not drinking or eating well.
Examination Kobi was wasted, having loose skin folds over his arms, buttocks and thighs and visible ribs outlined. Vital signs: temperature: 34.8o C, pulse: 130/min, RR: 50/min Weight: 6.0 kg and Length: 69cm, MUAC 10.5cm □ UseTable 35 p. 386 and assess Kobi’s weight-for-length and weight-for-age (p. 385) Chest: air entry was normal both sides, front and back Cardiovascular: both heart sounds were heard and there was no murmur Abdomen: soft, bowel sound was audible; no organomegaly Ears-Nose-Throat: dry mucus membranes Eyes: sunken, no tears and dry conjunctiva Skin: decreased skin turgor Neurology: sick looking; no neck stiffness and no other focal signs
X (p. 385)
Differential diagnoses • Severe malnutrition (marasmus) due to inadequate food intake • Severe malnutrition due to other organic disease: Tuberculosis HIV Malabsorption syndrome Other chronic disease Micronutrient deficiency (Vitamin A, zinc) (Ref. p. 198-199)
Additional questions on history • Nutrition history from birth • Duration and frequency of diarrhoea and vomiting • Type of diarrhoea (watery / bloody/ mucous / pus) • Family circumstances and home environment • Chronic cough • Contact with TB, measles • Known or suspected HIV
Nutritional history Kobi had been on formula feed since 4 months of age. The milk was diluted (one scoop of milk per whole bottle of water). His mother would wash his bottles and teats in tap water. He was given weaning food at six months of age, mainly contained potato and occasional vegetables. He would get meat occasionally, but not for the past 2 months. He usually receives two meals and two bottles of milk each day. Kobi has to share his plate of food with his other siblings.
Family circumstances Kobi lives with his parents in a small wooden house. He has 3 older sisters and 2 older brothers. They have a small plot of land on which they grow crops, but which is not sufficient to feed their family. Kobi’s father works as a farmer and his mother as a housemaid where they can earn some more money for food. Because they are busy, Kobi’s older siblings mostly take care of him.
Further examination of a child with severe malnutrition Look for: • Severe palmer pallor • Eye signs of vitamin A deficiency • Skin changes of kwashiorkor • Localising signs of infection • Signs of HIV • Fever or hypothermia • Mouth ulcers • Signs of dehydration (Ref. p. 199)
Further examination Palmer Pallor – indicates anaemia (Ref. p. 166). In any child with palmer pallor, check the haemoglobin or haematocrit level Check conjunctiva and mucous membranes
Further examination Look for signs of vitamin A deficiency: • Dry conjunctiva or cornea • Bitot spots • Corneal ulceration • Keratomalacia (Ref. p. 199)
Investigations • Blood glucose: 2.4 mmol/L (3-6.5mmol/L) • Haemoglobin: 70 g/l (105-135) • Chest x-ray: normal, no features of TB • Stool microscopy shows trophozoites of giardia • After counseling of parents, HIV PCR test - negative
Diagnosis • Severe malnutrition, with complications: hypothermia, hypoglycaemia • Anaemia • Giardia infection causing diarrhoea
Treatment10 steps in 2 phases:initial stabilization and rehabilitation (Ref. p. 201)
Step 1: prevent hypoglycaemia □ Hypoglycaemia (Ref. p. 201): give the first feed of F-75. If it is not available give 50ml of 10% glucose solution orally or by nasogastric tube give 3 hourly feeds At least 6 feeds per day Day and night for the 2 days After day 2, give at least 6 feeds during day (e.g. 0600, 0900, 1200, 1500, 1800, 2100) and overnight if possible
Step 2: prevent hypothermia □ Hypothermia (Ref. p. 202-203): immediate and 3 hour feeding reduces risk of hypothermia and hypoglycaemia make sure the child is clothed (including the head), use warmed blanket or put the child on the mother's bare chest or abdomen
Step 3: if there is dehydration □ If there is dehydration (Ref. p. 203-204): give rehydration solution orally or by nasogastric tube, much more slowly than you would when rehydrating a well-nourished child if rehydration is still occurring at 6 hours give the same volume of starter F-75 instead of ORS at these times Refer to Ref. p. 203-204 or PNG malnutrition guidelines for details
Step 4: electrolytes □ Electrolytes (Ref. p. 206): If electrolytes are not added to the food, give: zinc (10 mg/day if <10 kg ; 20mg/day >10kg) potassium (3-4mmol/kg/day) magnesium (0.4-0.6mmol/kg/day) prepare food without salt • If F-75 is provided there is no need to add electrolytes to food • Refeeding syndrome is a big risk in the first week
Step 5: treat infection □ Infection (Ref. p. 207-208): give all severely malnourished children who are unwell broad-spectrum antibiotic (penicillin & gentamicin) in Kobi’s case treat also for giardia (metronidazole: 5mg/kg, 3 times a day, for 5 days (Ref. p. 137)) or Tinidazole for 3 days give measles vaccine if the child is not immunized
Step 6: micronutrients □ Micronutrients (Ref. p. 208-209): If micronutrients are not added to the food: give daily multivitamins give vitamin A orally on day 1 once gaining weight, give ferrous sulfate give iron only after the child gains weight, because iron can make infections worse
Step 7: initiate feeding □ Initiate feeding (Ref. p. 209-210): give F-75 (or Full Strength Sunshine milk) 100kcal/kg/day (liquid: 130ml/kg/day; protein: 1-1.5g/kg/day) 3 hourly feeds At least 6 feeds per day Day and night for the first 2 days After day 2, give 6 feeds during day (e.g. 0600, 0900, 1200, 1500, 1800, 2100) and overnight if possible continue breastfeeding if possible in addition
Step 8: catch up growth □ Catch-up growth(Ref. p. 210-215): replace the starter F-75 with F-100 or Milk Oil Formula. Use RUTF also if the child is older than 6 months use the same amount of F-100 as F-75 for 2 days then increase each feed until some food remains uneaten (up to 220 ml/kg/day) continue breastfeeding if possible in addition
Step 9: sensory stimulation □ Sensory stimulation (Ref. p. 215): provide loving care, a friendly stimulating environment and involvement of the mother toys for the child to play with or books to look at physical activity as soon as the child is well enough
What is happening? What would you do?
Monitoring Monitor for complications: Heart failure (Ref. p. 214) Infection Hypothermia Hypoglycaemia Dehydration Refeeding syndrome
Monitoring • Weigh the child the same time of the day, after removing clothes (Ref. p. 222-223) • Calculate weight change and plot weight on chart (Ref. p. 215) • Weigh every 2nd day • Record the weight gain: • >10g/kg/day – good • 5-10g/kg/day – moderate • <5g/kg/day – poor • E.g, a 6kg child should gain more than 6 x 10g x 7 days = more than 420 g per week • An 8.5kg child should gain more than 8.5 x 10g x 7 days = 595 g per week
Monitoring • If weight gain is poor check the following points: • Inadequate feeding – give more, observe the child feeding, consider need for a nasogastric tube • Untreated infection? • Another illness, such as HIV/AIDS? • Emotional or psychological problems
Discharge and follow-up (Ref. 219-222) Before discharge the child should have: • Completed antibiotic treatment • Regained a good appetite, taking all feeds regularly • Show good weight gain (weight gain >70g/kg/week and Z-score > -2 SD) The mother or carer should: • Be available for child care • Have received training on appropriate feeding • Have enough resources at home to feed the child
Follow-up • Make a plan for the follow-up of the child until complete recovery • The child should be weighed weekly after discharge. • If the child does not gain weight over 2-week period or it even lost weight, he should be referred back to hospital.
Progress • Kobi was discharged after gaining weight and regaining appetite • His parents were told to feed him at least 5 times per day. They had to give him high-energy snacks between meals (e.g. milk, banana, bread, biscuits). • His parents were told to encourage him to complete each meal, to add micronutrient supplements to each feed, continue iron for 3 months, and to monitor his appetite and intake. • His mother was encouraged to breastfeed him as often as Kobi wants. • Follow-up was arranged. • Kobi still needs continuing care as an outpatient to complete rehabilitation and prevent relapse.
Summary • 12 month old, youngest in family of 6. Early weaning, diluted formula, poorly nutritious food, repeated infections, diarrhoea and anaemia • Severe malnutrition with hypothermia, hypoglycemia, anaemia, giardiasis • HIV negative, no signs of TB • Malnourished children have multiple medical, social and psychological problems, and each need to be identified and addressed • Family completion was discussed with Kobi’s mother and father