Download
1 / 8
80 likes | 203 Views
Manifestations of Severe Malnutrition. Juliana E. Reeves Oct. 15, 2004 ACR code 73.79. 29 yo F Presented to OSH on 9/15 with chronic abdominal pain, nausea, vomiting 2mo h/o 40 lb wt loss 1mo h/o plugged PEG Emaciated, mild abdominal tenderness, no rebound, skin breakdown around PEG

E N D
Manifestations of Severe Malnutrition Juliana E. Reeves Oct. 15, 2004 ACR code 73.79
29 yo F • Presented to OSH on 9/15 with chronic abdominal pain, nausea, vomiting • 2mo h/o 40 lb wt loss • 1mo h/o plugged PEG • Emaciated, mild abdominal tenderness, no rebound, skin breakdown around PEG • LFT wnl except albumin of 1.6 and protein of 3.7 • Lipids, Vit A & D and folate decreased
Past Medical History • 9 yr h/o chronic abdominal pain, with intermittent nausea and vomiting • s/p Laparoscopy Jan. 1999 • s/p Lap Chole and Appy in 2000 • s/p PEG tube placement Feb. 2002 • Prior records show a possible diagnosis of irritable bowel syndrome, multiple medications provided no relief
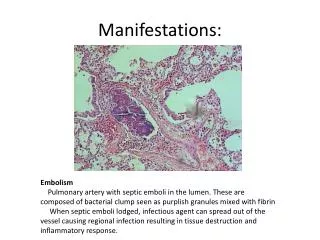
Radiographic Features & Differential Diagnosis Radiographic Features • Marked hepatic steatosis (diffusely hypodense) by CT • Scissoring of duodenum between aorta and SMA • Narrowing of duodenum by upper GI Differential Diagnosis • SMA syndrome/Wilkie’s syndrome • Anorexia Nervosa • Duodenal Obstruction • Pancreatitis
Discussion • First described by von Rokitansky in 1861 • Compression of duodenum between aorta and SMA, leading to obstruction and dilatation • Wasting diseases, rapid weight loss and extreme lordosis can contribute to its development • Postprandial epigastric pain and fullness are relieved by vomiting • Can simulate or complicate anorexia nervosa • Occurs most commonly in young adult women
References • Adson, David E et al. The Superior Mesenteric Artery Syndrome and Acute Gastric Dilatation in Eating Disorders: A Report of Two Cases and a Review of the Literature. International Journal of Eating Disorders 1997; 21:103-14. • Kwan, Eugene et al. Wilkie’s Syndrome. Surgery 2004; 135:225-7. • Lim, Jonathon E et al. Superior Mesenteric Artery Syndrome Presenting with Acute Massive Gastric Dilatation, Gastric Wall Pneumatosis, and Portal Venous Gas. Surgery 2003; 134:840-3. • Payawal, Jonathon H et al. Superior Mesenteric Artery Syndrome Involving the Duodenum and Jejunum. Emergency Radiology 2004; 10:273-5.