Download
1 / 28
760 likes | 1.86k Views
Alcohol Metabolism. Most toxicologists consider ethanol to be the most often used and abused chemical substance The measurement of ethanol is one of the more frequently performed tests in the toxicology laboratory

E N D
Most toxicologists consider ethanol to be the most often used and abused chemical substance • The measurement of ethanol is one of the more frequently performed tests in the toxicology laboratory • When alcohol consumed with other CNS depressant drugs, ethanol exerts a potentiation or synergistic depressant effect • Ethanol absorbed to a small extent in the stomach and mainly by the upper small intestine • After the consumption of alcohol blood alcohol concentration peaks within 30 to 45 minutes
Alcohol cannot be stored and has priority in metabolism • Through oxidation, alcohol is detoxified and removed from the blood, preventing the alcohol from accumulation and destroying cells and organs • Some ethanol are metabolized by the stomach cells • Most of the alcohol consumed is metabolized in the liver, but the small quantity that remains unmetabolized permits alcohol concentration to be measured in breath and urine • Alcohol is metabolized more slowly than it is absorbed
Factors Influencing Alcohol Absorption and Metabolism • Food: • The presence of food • Type of food • Gender: • Females are more susceptible to alcohol toxicity than males
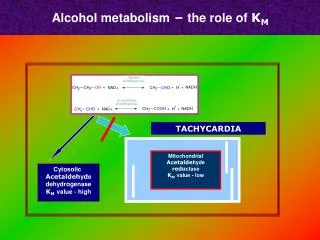
Conversion of ethanol to acetaldehyde • Catalyzed by alcohol dehydrogenase IB a member of the alcohol dehydrogenase family • Consisting of several homo- and heterodimers of alpha, beta and gamma subunits • The rate-determining reaction in ethanol metabolism • This family of enzymes metabolize a wide variety of substrates • Ethanol • Retinol • Hydroxysteroids • Lipid peroxidation products • Other aliphatic alcohols
ADH • 5 different isoforms are present ADH1 to ADH5. • The ADH2 isoform is commonly called ‘atypical’ ADH. • This isoform contains a variant beta2 subunit instead of the usual beta1 subunit. beta2 has much higher activity than beta1.
Conversion of acetaldehyde to acetic acid • The enzyme responsible for this conversion is aldehyde dehydrogenase II, this enzyme belongs to the aldehyde dehydrogenase family of protiens • Two major liver isoforms of this enzyme: • Cytosolic • Mitochondrial • These two isoforms can be distinguished by their: • Electrophoretic mobilities • Kinetic properties • Sub-celellular localizations
Acetaldehyde • Far more toxic than ethanol. • Acetaldehyde is a highly unstable compound and quickly forms free radical structures • The injury ; from fatty infiltration to fibrosis and if the hepatocellular necrosis and liver insult continue, cirrhosis and even death. • The fibrosis and cirrhosis are irreversible. • Alcohol sensitivity symptoms is all due to the inability to metabolize acetaldehyde and NOT ethanol.
Metabolic fates of NADH • Conversion of pyruvic acid to lactic acid: • Lactic acid build-up; Acidosis • Lack of glucose synthesis;Hypoglycemia • Synthesis of lipids: • Synthesis of glycerol • Synthesis of fatty acids • Electron transport chain: • ATP synthesis • Fats accumulation • Acetyl CoA accumulation with ketone bodies formation
Microsomal ethanoloxidizing system (MEOS) • Excessive alcohol intake, ADH cannot keep up with demand • Used to metabolize drugs, foreign substances in addition to alcohol • Involving cytochrome P450 especially CYP2E1 • CYP1A2 and CYP3A4 are also involved • Chronic ethanol consumption increases the activity of MEOS including CYP2E1 • CYP2E1 activates • Catabolism of acetaminophen to their toxic metabolites • Accelerates catabolism of retinol resulting in its depletion • Significant release of free radicals, diminishes reduced glutathione (GSH)
Fate of Acetyl-CoA CO2 + H2O Acetyl-CoA Fatty Acid X Glucose
Effects of alcohol metabolism • Body weight: drinkers were not more obese than nondrinkers • Sex hormones: alcohol metabolism alters the balance of reproductive hormones in men (impairs testosterone synthesis and sperm production) and women (increase production of estradiol) • Medications: activation the enzyme CYP2E1, which may be responsible for the transformation of many drugs into chemicals that can cause liver damage
Why some people develop alcoholism and others do not??? • Alcohol dehydrogenase genes may be associated with differential resistance and vulnerability to alcohol • Alternate paths of alcohol metabolism
Oxidation of alcohol takes precedence over other metabolic pathways • Elevated NADH + H+, which favors rx’s which require NADH + H+ • Synthesis of glycerol-PO4 • pyruvate ------> lactate • acetyl-CoA-----> citrate-----> fatty acids • Fatty infiltration of liver due to excessive alcohol consumption: 1) Decrease fat oxidation 2) Increase lipogenesis 3) Decrease lipoprotein release
Proteins: 1) Inhibit protein synthesis in brain 2) High concentration of ethanol can inhibit the absorption of some amino acids. • Isoleucine, • Arginine, and • Methionine • Micronutrients: 1) Poor intake 2) Changes in • Absorption • Storage • Metabolism • Excretion
Folate deficiency due to: 1) Decrease absorption 2) Decrease hepatic uptake or storage 3) Increase urinary excretion -Leading cause of anemia in alcoholics • Thiamin: • impaired intestinal absorption • Pyridoxine (B6): 1) Decrease hepatic stores 2) Increase urinary loss
Vitamin A: 1) Decrease hepatic storage, especially with cirrhosis 2) Possible increase in vitamin A metabolism in microsomes, causing increase retinoic acid 3) Malabsorption as a fat-soluble vitamin -Decrease in cellular differentiation which promotes tumor growth •Zinc: 2) Impaired absorption 3) Increase urinary excretion • Selenium and Vitamin E: 1) Slight decrease in plasma concentration
Damage to the GI Tract • Damage the cells, inflammation of the stomach, oesophagus, and intestines • Malabsorption • Diarrhea and steatorrhea • Inflammation of the pancreas and gall bladder – Decrease enzyme production – Disturbance in bile excretion • Difficulty digesting (and absorbing) nutrients
Cardiovascular Disease (CVD) • Moderate consumption of alcohol can increase HDL levels, which can reduce the risk of CVD ?? • HDL protects against the deposition of arterial fatty plaque
Cirrhosis • Fatty infiltration of the liver • Response to increased synthesis of fat from accelerated acetyl-CoA production • Enlarge fat cells chokes off nutrients and O2 supply to liver cells • Engorged fat cells burst and die • Scar tissue • 50% chance of death within 4 years
Brain Damage • Cognitive dysfunction and motor nerve deficit • Shrinks the brain • Reduces oxygen and nutrients to the brain • Alcohol is a powerful depressant