Download
1 / 118
1.19k likes | 1.44k Views
Module 2: Diagnosis of BPH. Luc Valiquette, MD, FRCSC Professor of Surgery, Urology Department of Surgery, Université de Montréal Chief of Urology at Centre Hospitalier de l’Université de Montréal Montréal, Québec. 2.1 Learning Objectives.

E N D
Module 2: Diagnosis of BPH Luc Valiquette, MD, FRCSCProfessor of Surgery, Urology Department of Surgery, Université de MontréalChief of Urology at Centre Hospitalier del’Université de MontréalMontréal, Québec
2.1 Learning Objectives • After reviewing this module, the learner will be better able to: • Perform the differential diagnosis and alarm features used to identify benign prostatic hyperplasia (BPH) • Identify which diagnostic assessments are appropriate at the initial evaluation of a typical patient with lower urinary tract symptoms (LUTS) • Identify which optional diagnostic assessments are appropriate in selected patients BPH = Benign Prostatic Hyperplasia; LUTS = Lower Urinary Tract Symptoms
After reviewing this module, the learner will be better able to: • Access clinical practice tools to evaluate BPH symptoms • Implement CUA diagnostic algorithms in daily clinical practice • Understand the appropriate roles of the family physician and recognize the time for specialist referral BPH = Benign Prostatic Hyperplasia; CUA = Canadian Urological Association
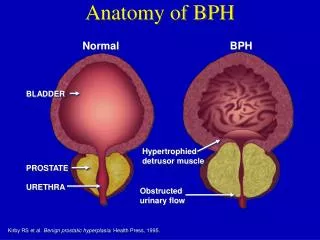
2.2 Introduction • Benign prostatic hyperplasia (BPH) is a naturally progressing, histologic disorder. The most prevalent condition to affect the prostate, it accounts for over 80% of clinical presentations for prostate disease.1 • Most men who visit their physicians for prostate-related problems want to be reassured that they do not have prostate cancer. 1. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p21.
In the course of a basic evaluation to rule out this disease, BPH may be detected by symptomatology and, if the patient is willing, DRE and serum PSA analysis. • Over 40% of men beyond the age of 69 have lower urinary tract symptoms (LUTS) and about half this group has an impaired quality of life2 • The only definitive way to confirm the presence of BPH is by biopsy; however, this procedure is usually regarded as unnecessary and is not part of a routine assessment. 2. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p21. BPH = Benign Prostatic Hyperplasia; DRE=Digital Rectal Examination; PSA=Prostate-Specific Antigen
This module will review the diagnostic evaluations that are appropriate for the initial assessment of a typical man >50 years of age who presents with LUTS and who is suspected of having BPH. • It will focus on evaluations recommended by the Canadian BPH Guidelines. • Note that a specialist in Urology should be consulted to assess the man with LUTS under 50 to determine the etiology of the symptoms in order to provide greater assurance that there is no cancer, stricture or other problem. BPH = Benign Prostatic Hyperplasia; LUTS = Lower Urinary Tract Symptoms
In addition, this module reviews the differential diagnosis of BPH, with particular reference to the differentiation of BPH from prostate cancer, and guidelines for primary-care physicians that suggest when to refer patients with BPH to an urologist for assessment. • The diagnostic algorithms and symptom assessment tools may be used in clinical practice to guide the diagnosis of BPH. BPH = Benign Prostatic Hyperplasia
2.3 Initial Evaluation • This section will explore the diagnostic tests that are appropriate to conduct during the initial visit of a typical patient, i.e., man >50 year of age who complains of LUTS • The following diagnostic evaluations are described here: • Medical history • Lower urinary tract symptoms (LUTS) • Physical examination • Digital rectal examination (DRE) • Diagnostic tests • Urinalysis • Prostate-specific antigen (PSA) measurement
Medical History • During the initial evaluation of a typical patient >50 years of age who presents with lower urinary tract symptoms (LUTS), a medical history can identify other causes of voiding dysfunction or concomitant medical conditions that may complicate treatment3 • Key elements of the medical history include:4,5 • Focus on urinary tract • Identification of LUTS • Severity and bother of symptoms • Previous surgical procedures • History of trauma 3. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p21. 4. AUA guideline on management of benign prostatic hyperplasia (2003) J. Urol. 2003;170:530-547. 5. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol. 2005;12:2582-88
Key elements of the medical history cont’d:6,7 • General health issues • Sexual dysfunction • Concomitant medical conditions that may lead to bladder dysfunction or excessive urine output • Family history of prostate diseases, including BPH and cancer • Current medications, including OTC products • Fitness for surgery 6. AUA guideline on management of benign prostatic hyperplasia (2003). J Urol. 2003;170:530-547. 7. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol. 2005;12:2582-88 OTC = Over the Counter
The Identification of LUTS • BPH is characterized by a spectrum of obstructive and irritative symptoms, known as LUTS (see Table 2.1) 8 • However, other lower urinary tract disorders may produce similar, if not identical, symptoms in aging men9 • LUTS may occur in men with prostate cancer, prostatitis, or many other medical disorders10 8. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p21. 9.Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p19. 10. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p21. BPH = Benign Prostatic Hyperplasia; LUTS = Lower Urinary Tract Symptoms
A detailed discussion of the differential diagnosis for BPH appears in section 2.6 • The major categories are summarized as follows: • Dribbling after micturition • Concomitant medical conditions • Prostate cancer BPH = Benign Prostatic Hyperplasia
In a significant number of men, non-prostatic causes of LUTS can be excluded on the basis of a medical history, physical examination, and urinalysis11 • The severity of LUTS can be objectively measured by the following clinical assessment tools: • International Prostate Symptom Score (IPSS) (or alternatively American Urological Association (AUA) symptom index) • Disease-specific Quality of Life (QoL) questionnaire • BPH Impact Index 11. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p19. LUTS = Lower Urinary Tract Symptoms
Table 2.1: BPH Related LUTS12,13* *Note: some experts question the value of categorizing LUTS as obstructive or irritative 12. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p21.13. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p19.
Practice Tip • Prostate symptom scores offer a more objective measure of LUTS14 • Practice Tip • To avoid interviewer bias, ask patients to self-administer symptom questionnaires. • Some clinicians find it efficient to ask patients with LUTS to complete the questionnaires in the waiting room before seeing them, or complete the forms before the next visit. 14. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p19.LUTS = Lower Urinary Tract Symptoms
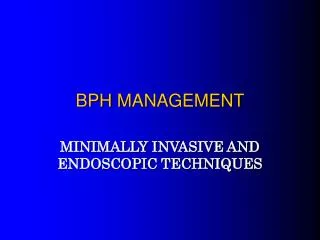
Physical Examination • The physical examination must include a digital rectal examination (DRE) and focused neurological assessment.15 The physical examination is considered mandatory15,16 • The neurological examination should assess:17,18,19 • General mental status • Ambulatory status • Lower extremity neuromuscular function • Bulbocavernosal reflex (if neurologic disease is suspected) • Anal sphincter tone • Overall motor and sensory function 15. AUA guideline on management of benign prostatic hyperplasia (2003).J.Urol. 2003;170:530-547. 16. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol. 2005;12:2582-88. 17. AUA guideline on management of benign prostatic hyperplasia (2003).J Urol. Publication, 2001:523. 18. Chatelain C et al.Plymouth, UK: Health Publication, 2001:523. 19. Jepsen JV, Bruskewitz RC. Urol Clinics N Am. 1998;25:547.
Neurological findings may strongly suggest the presence of a neurogenic bladder20 • The absence of neurological findings may help to exclude nervous system disorders, such as Parkinson’s disease or a cauda equina lesion, as the underlying cause of LUTS21 20. Jepsen JV, Bruskewitz RC. Urol Clinics N Am. 1998;25:547. 21. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25. LUTS = Lower Urinary Tract Symptoms
In addition to the DRE, the focused physical examination should include22: • Palpation and percussion of abdomen and costovertebral angles to clinically exclude: • Hydronephrosis • Pyelonephritis • Renal mass • Bladder dilation • Suprapubic palpation and percussion to exclude bladder distension or other mass lesion:23,24,25 • Palpable bladder may indicate significant residual urine and advanced BPH 22. Jepsen JV, Bruskewitz RC. Urol Clinics N Am. 1998;25:547. 23. Chatelain C et al. Plymouth, UK: Health Publication, 2001:523. 24. Jepsen JV, Bruskewitz RC. Urol Clinics N Am. 1998;25:547. 25. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p21-22. DRE = Digital Rectal Examination; BPH = Benign Prostatic Hyperplasia
The physical examination should also include: • Assessment of general appearance26 • Skin colour and turgor • Body weight, posture, build • Edema, as a sign of renal insufficiency 4. Genital examination27 • Routine palpation of penis, urethra, testicles and epididymis to rule out unrelated disease processes 26. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p21-22. 27. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p21-22.
Practice Tip • Urinary tract infections in older men may indicate significant BPH and bladder outlet obstruction28 • Practice Tip • Abdominal examination rarely identifies pathology but when abnormalities are discovered it is usually very significant29 28. Jepsen JV, Bruskewitz RC. Urol Clinics N Am. 1998;25:547. 29. Jepsen JV, Bruskewitz RC. Urol Clinics N Am. 1998;25:547. BPH = Benign Prostatic Hyperplasia
Digital Rectal Examination (DRE) • The digital rectal examination (DRE) is the cornerstone of the physical examination when BPH is suspected30 • The primary purpose of this examination is to rule out prostate cancer, which also produces LUTS31 • The DRE provides useful clinical information for the diagnosis of BPH (see Table 2.2) 32 • For the DRE, the patient can lie in a left lateral or knee-elbow position33 30. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25. 31. AUA guideline on management of benign prostatic hyperplasia (2003).J Urol. 2003;170:530-547. 32. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25. 33. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25.LUTS – Lower Urinary Tract Symptoms; BPH = Benign Prostatic Hyperplasia
The DRE estimates prostate34,35 • Size • Consistency • Symmetry • Smoothness • Tenderness • Anatomical limits • The DRE can identify abnormalities suggestive of prostate cancer:36 • Nodules • Irregularities • Firmness 34. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25. 35. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p21-22. 36. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p21-22.
From the DRE, physicians can estimate the volume of prostates of ≤50 cm3 with reasonable accuracy37 • This examination tends to underestimate the volume of larger glands, but if the prostate feels large on DRE, it is usually found to be enlarged by ultrasound or other means of measurement38,39 37. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25. 38. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25. 39. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p21-22.
Figure 2.1: Possible Findings on DRE Normal Tenderness Symmetrical Enlargement (BPH) Asymmetry Nodularity Induration DRE = Digital Rectal Exam
Table 2.2: Clinical Findings of DRE40,41 40. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25.41. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p21-22.
Diagnostic Tests Urinalysis • Urinalysis by dipstick or microscopic examination of urinary sediment is mandatory to screen for:42,43,44 • Hematuria • Urinary tract infection (UTI) • Proteinuria • Pyuria • Other pathological findings, e.g., glucose • A positive dipstick test is an indication for urine microscopy and culture, and further evaluation and imaging of the renal tract should be considered (see Table 2.3) 45 42. Nickel JC et al. Canadian guidelines for the management of benign prostatic hyperplasia. Can J Urol. 2005;12:2582-88. 43. AUA guideline on management of benign prostatic hyperplasia (2003).J Urol. 2003;170:530-547. 44. Chatelain C et al. Plymouth, UK: Health Publication, 2001:523. 45. Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p25.
Table 2.3: Findings of Urinalysis46 46. Ramsey EW, McSherry J. A community care program on benign prostatic hyperplasia: a primary-care physician’s guide. Mississauga, ON: Astra Pharma Inc., 1996, p24. UTI – Urinary Tract Infection
Prostate-specific Antigen (PSA) • Serum prostate-specific antigen (PSA) is a predictor of the natural history of BPH • Serum PSA levels gradually increase over time • Men with higher PSA levels have a greater risk of prostate growth in future47 47. AUA guideline on management of benign prostatic hyperplasia (2003).J Urol. 2003;170:530-547. BPH = Benign Prostatic Hyperplasia
Figure 2.2: PSA Predicts Prostate Growth PSA tertiles (ng/ml) Prostate Growth (baseline %) Time (months) Adapted from Roehrborn CG et al. J Urol 2000;163:13-20. PSA = Prostate Specific Antigen
PSA testing, with the DRE, is a relatively sensitive way to rule out prostate cancer in aging men48 • However, the specificity of PSA testing for BPH is a confounding issue. • An overlap in diagnostic values exists for men with BPH and those with localized prostate cancer49 • For that reason, PSA levels should not be interpreted alone but together with findings of the DRE50 48. Nickel JC et al. Canadian Guidelines for the Management of Benign Prostatic Hyperplasia. Can J Urol. 2005;12:2582-88. 49. AUA guideline on management of benign prostatic hyperplasia (2003).J Urol. 2003;170:530-547. 50. AUA guideline on management of benign prostatic hyperplasia (2003).J Urol. 2003;170:530-547. PSA = Prostate-Specific Antigen; DRE = Digital Rectal Examination
Guidelines for Early Detection of Prostate Cancer DRE and PSA Tests • Increase the early detection of prostate cancer • Are indicated when prostate cancer is suspected • Are indicated in the management of prostate cancer • May help decide on treatment CUA 1996; www.cua.org/guidelines/earlydetection.htmlCPSM 1995; www.umanitoba.ca/academic/colleges/cps/guidelines_and_statements/317.html; CMQ 1998; www.cmq.org/Prostateang.pdf DRE = Digital Rectal Examination; PSA = Prostate-Specific Antigen
Other factors can elevate or suppress serum PSA levels, leading to false values, including:51 • Prostatitis • Sexual activity • Infection • Medications • Patients should be informed of the risks and benefits of PSA measurement52 51. American Urology Association. Oncology. 2000;14:267-286. 52. AUA guideline on management of benign prostatic hyperplasia (2003).J Urol. 2003;170:530-547. PSA = Prostate-Specific Antigen
PSA Testing – Yes or No? www.umanitoba.ca/academic/colleges/cps/guidelines_and_statements/3.17.html;Sarkar P, et al. Int J Pharm 2002; 238(1-2):1-9;Gander L (HSURC) 2000;www.hsurc.sk.ca; AUA. Oncology 2000;14:267-86;CMQ 1998;www.cmq.org/Prostateang.pdf;CPSM 1995.
When to Test Serum PSA • The PSA test is recommended for:53 • Patients who have at least a 10 year life expectancy and for whom knowledge of the presence of prostate cancer would change management • Men for whom PSA measurement may change the management of their voiding symptoms (by the estimation of prostate volume) 53. Nickel JC et al. Canadian Guidelines for the Management of Benign Prostatic Hyperplasia. Can J Urol. 2005;12:2582-88. PSA = Prostate-Specific Antigen
75 70 65 60 55 50 45 40 35 30 70 65 60 55 AGE (years) 50 Prostate Volume (cc) 45 40 1 2 3 4 5 6 7 8 Serum PSA, ng/ml Figure 2.3: Prediction of Average Prostate Volume Based Upon Serum PSA and Age Adapted from Roehrborn CG et al. Urology 1999;53:581-589. PSA = Prostate-Specific Antigen
PSA and Progression • Serum PSA measurement can be used as a biomarker for BPH disease progression • Men with symptoms and a PSA of ≥1.4 ng/mL are more likely to have a larger prostate (> 30 cc) with progressive BPH, deteriorating symptoms and urinary flow rate over time, and a higher risk of acute urinary retention and future surgery 54 • Men with symptoms and a serum PSA of <1.4 ng/mL are more likely to have a smaller prostate (<30 cc) and a lower likelihood of disease progression55,56 54. Roehrborn CG et al for the PLESS group. Urology. 1999;54:662-9. 55. Roehrborn CG et al for the PLESS group. Urology. 1999;54:662-9. 56. Bartsch G et al. BJU International. 2004;93(S1):27-9. PSA = Prostate-Specific Antigen; BPH = Benign Prostatic Hyperplasia
0.0 PSA 3.3 – 12 ng/mL PSA 1.4 – 3.2 ng/mL -1.0 -2.0 Quasi-AUA symptom score mean change ± SE PSA 0 – 1.3 ng/mL -3.0 -4.0 -5.0 0 1 2 3 4 Years on Study Figure 2.4: PSA and Symptoms*,** *Symptom scores (mean ± 95% confidence interval) stratified by baseline serum PSA.**Data from the 4-year, randomized, placebo-controlled PLESS study in which a total of 3040 men with BPH were enrolled and assigned to once-daily finasteride 5mg or placebo. Symptoms and flow rate were assessed every 4 months, and data were analyzed by dividing the placebo-treated patients into 3 groups by baseline PSA tertiles (0 to 1.3, 1.4 to 3.2, and 3.3 ng/mL or greater). Quasi-AUA = the symptom score based on an adaptation of the American Urological Association symptom scale; BPH= benign prostatic hyperplasia; PLESS = Proscar Long-Term Efficacy and Safety Study; PSA = prostate-specific antigen; SE=standard error. Adpated from Roehrborn CG et al. Urology 1999;54(4):662-9.
Figure 2.5: Bother and PSA 0 -0.5 -1 -1.5 -2 -2.5 -3 PSA tertiles(ng/mL) Mean (SE) changein bother score PSA 0 – 1.3 PSA 1.4 – 3.2 PSA 3.3 - 12 0 1 2 3 4 Year of follow up Adapted from Bruskewitz R et al. Urology 1999;54:670-678. ; PSA = Prostate-Specific Antigen
Figure 2.6: Peak Flow Rates and PSA Months 0 4 8 12 16 20 24 28 32 36 40 44 48 1.5 1 0.5 0 -0.5 -1 -1.5 PSA tertiles(ng/ml) PSA 0–1.2 PSA 1.3–3.2 PSA 3.2–10 Adapted from Roehrborn CG et al. Urology 1999;54:662-669. ; PSA = Prostate-Specific Antigen
Baseline PSA tertiles PSA 0–1.2 ng/ml PSA 1.3–3.2 ng/ml PSA >3.2 ng/ml Figure 2.7: Incidence of Surgery and AUR over 4 years by PSA Tertiles 21 (Placebo-treated BPH) 18 14.6% 15 Incidence (%) 12.6% 12 9.9% 9 6.2% 5.8% 6 2.9% 3 0 Surgery AUR Adapted from Roerhborn CG. AUA 2005.
7 5.9 6 5 4.5 4 3.1 2.8 3 1.8 2 1 0.8 1 0.3 0 Overall Symptom AUR Inv. Therapy Progression Progression Figure 2.8: MTOPS Subanalysis PSA and Risk of BPH Progression p = 0.0008 p = 0.0251 <1.6 ng/ml ≥1.6 ng/ml Rate per 100 PYR p = 0.0180 p = 0.0029 McConnell JD et al. J Urol. 2003;169(suppl):332.
Practice Tip • The risk of BPH progression is higher in men with a PSA >1.4 ng/mL59 • Practice Tip • PSA alone is insufficient to detect localized prostate cancer60 59. Kirby RS. UK;Prostate Research Campaign UK, 2000, pp53. 60. Jepsen JV, Bruskewitz RC.Urol Clinics N Am. 1998;25:548. BPH = Benign Prostatic Hyperplasia; PSA = Prostate-Specific Antigen
Figure 2.9: Prostate-specific Antigen (PSA) and How it Gets into the Blood Stream Adapted from Kirby RS, McConnell JD. Benign Prostatic Hyperplasia. 5th ed. Oxford: Health Press, 2005, p28.
More Information About Serum PSA • A 4-year, multicentre study of 164 men with BPH in the placebo group of the Proscar Long-term Efficacy and Safety Study (PLESS) established that serum PSA is a stronger predictor of prostate growth than age or baseline prostate volume62 (Refer to Figure 2.2) 62. Roehrborn CG et al for the PLESS group. J Urol. 2000;163:13.BPH = Benign Prostatic Hyperplasia; PSA = Prostate-Specific Antigen
These men had an overall growth rate in prostate volume of 1.8cc per year. • Prostate growth increased steadily by 5.2% in the first year, 9.0% in the second year, 11.8% in the third year, and 14.1% in the fourth year. • In another analysis of the PLESS study, a strong association between prostate volume or PSA and the risk of acute urinary retention and a need for BPH-related surgery was demonstrated. • Serum PSA measurement was established as an important predictor of BPH-related outcomes. BPH = Benign Prostatic Hyperplasia; PSA = Prostate-Specific Antigen
Earlier analysis of PLESS placebo-group data showed that baseline PSA values and prostate volume are good predictors of long-term changes in symptoms and flow rate changes in men with BPH63 • Men with a PSA of ≥1.4 ng/mL and to a larger extent those with a PSA of ≥3.2 ng/mL were more likely to have a larger prostate with progressive BPH, a higher risk of acute urinary retention and future surgery, and deteriorating symptoms and urinary flow rate over time. 63. Roehrborn CG et al for the PLESS group. Urology. 1999;54:662-9. BPH = Benign Prostatic Hyperplasia; PSA = Prostate-Specific Antigen
Age-specific serum PSA reference ranges were first established in 1993, based on a 2-year study of a community-based population of 2119 healthy white men in Olmstead County, Minnesota, USA64 • This study determined that serum PSA concentration is directly correlated with patient age and prostate volume. 64. Oesterling JE et al. JAMA. 1993;270:860-4. PSA = Prostate-Specific Antigen
Subsequent studies found that PSA levels vary in different racial groups, with black men having higher PSA levels than whites65 65. Morgan TO et al. N Engl J Med. 1996;335:304-10. PSA = Prostate-Specific Antigen
Table 2.4: Relative Risk of Prostate Enlargement by PSA Level *Estimated by hazard function†The Wald chi-square statistic was used in the model to calculate p values for comparisons between a PSA quartile and reference (lowest) quartile. Wright JE et al. J Urol. 2002;167:2485. ; PSA = Prostate-Specific Antigen
An analysis of 4627 patients from BPH trials and a safety study confirmed that prostate volume is strongly related to serum PSA in men with BPH and no evidence of prostate cancer and that this relationship depends on age67 67. Roehrborn CG et al. Urology. 1999;53:581-9. BPH = Benign Prostatic Hyperplasia PSA = Prostate-Specific Antigen