Download
1 / 1
10 likes | 266 Views
Ealing Hospital NHS Trust Pregnancies that just do not go away Abdullah asma , Aboud Rima , Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom. INTRODUCTION

E N D
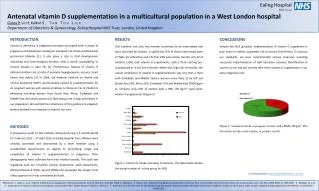
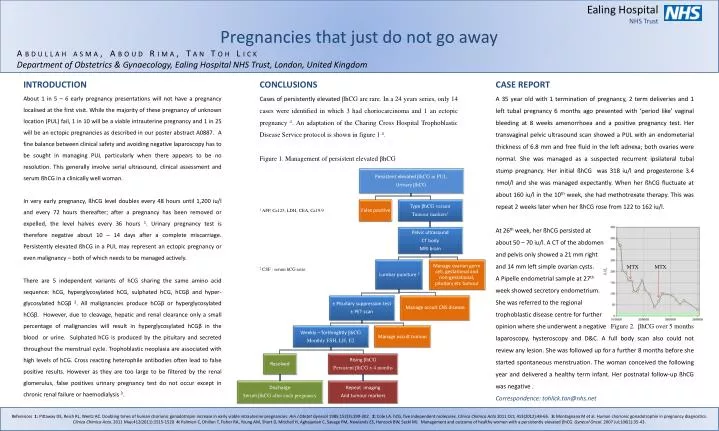
Ealing Hospital NHS Trust Pregnancies that just do not go away Abdullah asma, AboudRima, Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom INTRODUCTION About 1 in 5 – 6 early pregnancy presentations will not have a pregnancy localised at the first visit. While the majority of these pregnancy of unknown location (PUL) fail, 1 in 10 will be a viable intrauterine pregnancy and 1 in 25 will be an ectopic pregnancies as described in our poster abstract A0887. A fine balance between clinical safety and avoiding negative laparoscopy has to be sought in managing PUL particularly when there appears to be no resolution. This generally involve serial ultrasound, clinical assessment and serum ßhCG in a clinically well woman. In very early pregnancy, ßhCG level doubles every 48 hours until 1,200 iu/l and every 72 hours thereafter; after a pregnancy has been removed or expelled, the level halves every 36 hours 1. Urinary pregnancy test is therefore negative about 10 – 14 days after a complete miscarriage. Persistently elevated ßhCG in a PUL may represent an ectopic pregnancy or even malignancy – both of which needs to be managed actively. There are 5 independent variants of hCG sharing the same amino acid sequence: hCG, hyperglycosylatedhCG, sulphated hCG, hCGβ and hyper-glycosylatedhCGβ2. All malignancies produce hCGβ or hyperglycosylatedhCGβ. However, due to cleavage, hepatic and renal clearance only a small percentage of malignancies will result in hyperglycosylatedhCGβ in the blood or urine. Sulphated hCG is produced by the pituitary and secreted throughout the menstrual cycle. Trophoblasticneoplasia are associated with high levels of hCG. Cross reacting heterophile antibodies often lead to false positive results. However as they are too large to be filtered by the renal glomerulus, false positives urinary pregnancy test do not occur except in chronic renal failure or haemodialysis 3. CONCLUSIONS Cases of persistently elevated βhCG are rare. In a 24 years series, only 14 cases were identified in which 3 had choriocarcinoma and 1 an ectopic pregnancy 4. An adaptation of the Charing Cross Hospital Trophoblastic Disease Service protocol is shown in figure 1 4. Figure 1. Management of persistent elevated βhCG 1 AFP, Ca125, LDH, CEA, Ca19.9 2 CSF : serum hCG ratio CASE REPORT A 35 year old with 1 termination of pregnancy, 2 term deliveries and 1 left tubal pregnancy 6 months ago presented with ‘period like’ vaginal bleeding at 8 weeks amenorrhoea and a positive pregnancy test. Her transvaginal pelvic ultrasound scan showed a PUL with an endometerial thickness of 6.8 mm and free fluid in the left adnexa; both ovaries were normal. She was managed as a suspected recurrent ipsilateral tubal stump pregnancy. Her initial ßhCG was 318 iu/l and progesterone 3.4 nmol/l and she was managed expectantly. When her ßhCG fluctuate at about 160 iu/l in the 10th week, she had methotrexate therapy. This was repeat 2 weeks later when her ßhCG rose from 122 to 162 iu/l. At 26th week, her ßhCG persisted at about 50 – 70 iu/l. A CT of the abdomen and pelvis only showed a 21 mm right and 14 mm left simple ovarian cysts. MTX MTX A Pipelle endometrial sample at 27th week showed secretoryendometrium. She was referred to the regional trophoblastic disease centre for further opinion where she underwent a negative Figure 2. βhCG over 5 months laparoscopy, hysteroscopy and D&C. A full body scan also could not review any lesion. She was followed up for a further 8 months before she started spontaneous menstruation. The woman conceived the following year and delivered a healthy term infant. Her postnatal follow-up ßhCG was negative . Correspondence: tohlick.tan@nhs.net References 1: Pittaway DE, Reish RL, Wentz AC. Doubling times of human chorionic gonadotropin increase in early viable intrauterine pregnancies. Am J ObstetGynecol1985;152(3):299-302. 2: Cole LA. hCG, five independent molecules. ClinicaChimicaActa 2011 Oct; 413(2012):48-65. 3: Montagnana M et al. Human chorionic gonadotrophin in pregnancy diagnostics. ClinicaChimicaActa. 2011 May;412(2011):1515-1520 4: Palmieri C, Dhillon T, Fisher RA, Young AM, Short D, Mitchell H, Aghajanian C, Savage PM, Newlands ES, Hancock BW, Seckl MJ. Management and outcome of healthy women with a persistently elevated hCG. GynecolOncol. 2007 Jul;106(1):35-43.