Download
1 / 39
390 likes | 535 Views
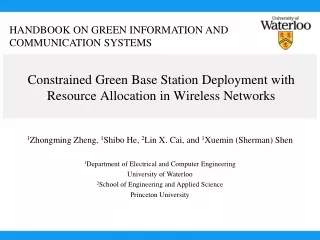
Designing Equitable Antiretroviral Allocation Strategies in Resource-Constrained Countries. David P. Wilson Sally M. Blower Presented by Harry Chang April 7 th , 2010. What is this about?. 2 Biomathematicians: UCLA AIDS Institute

E N D
Designing Equitable Antiretroviral Allocation Strategies in Resource-Constrained Countries David P. Wilson Sally M. Blower Presented by Harry Chang April 7th, 2010
What is this about? • 2 Biomathematicians: UCLA AIDS Institute • Topic: Equitable distribution of ARV in resource-constrained countries • Proposal: Mathematical model for achieving OEAS • Focus: KwaZulu-Natal province of South Africa
Outline • ARV Allocation Decision • Background • Experimental Outline • Methods • Results • Best Strategy • Future Extensions • Authors’ Conclusions
Reasons why I chose this topic • Caveats & Shortcomings • Discussed extensively: ARV for HIV/AIDS • Last presentation: ending note • Novel scientific approach • Interesting proposed resolution
Why did authors do this study? • ARV therapy expensive: barriers to providing essential medicines (eg. patents protecting IP), long-term treatment etc. • Cannot afford to treat all afflicted individuals • How to make decision?
Possible Strategies to Allocate ARV • Epidemiology • Preferential: • Men • Pregnant women • Children • Sickest • Highest efficiency • Military • Dominant ethnic group… • Lottery Peris, S.J. On a never-ending waiting list: toward equitable access to anti-retroviral treatment? Experiences from Zambia.Health and Human Rights, 8, 76-102. McGough LJ, Reynolds SJ, Quinn TC & Zenilman JM. Which patients first? Setting priorities for antiretroviral therapy where resources are limited. Am J Pub Heal, 95, 11173-1181.
WHO/UNAIDS ARV Distribution Policy • 1) All similar cases be treated alike • 2) Utilitarian: maximize overall social benefits • 3) Egalitarian: Equal distribution to different groups • 4) Maximin: Prioritize least advantaged individuals
Allocation Strategy Modelled in Study • Ethical: Equality • “Each individual with HIV has an equal chance of receiving ARV” • Intention: mathematical model of treatment accessibility & equity objective function OEAS
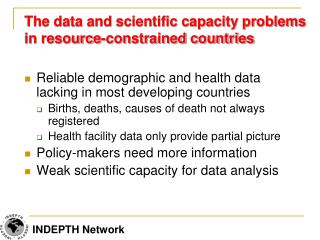
Province: KwaZulu-Natal • South Africa epidemic (12% of population) • KwaZulu-Natal = largest province • Population: 9.4 million • highest HIV-positive (21% of all South Africa) • Total HCF: 54
Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
South African ARV Roll-out Plan • April 2004 • 17 HCF in KwaZulu-Natal for ARV Roll-out • Variable distance between communities & HCF • Spatial distribution diverse heterogeneity, unequal accessibility to ARV
Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
Experimental Outline • Intention: Determine ARV OEAS for KwaZulu-Natal • Examine parameters • 1) Changing catchment region of HCF • 20km OR 40km OR 60km • 2) Number of HCF • 1 OR 17 OR 54 • Compare to • 1) All ARV to Durban • 2) Equal ARV to 17 HCF (current government plan)
Authors’ Assumptions • ARV available for distribution only treat 10% of infected • Catchment region: do not know hence approx 40km • Distance from community to HCF is determinant of whether patient has access to treatment • HIV prevalence: urban = 13%, rural = 9% • Only 51 communities in KwaZulu-Natal • Population > 500
1) Demand & Access • Accessibility = how likely a patient will travel to a HCF to receive ARV • # Patients go to HCF: increase with # of patients, decrease with distance
1) Demand & Access Con’t • Considered: • # people in community • Treatment Accessibility function • Gaussian • Radius of catchment region • Weighting function: distance btw community and HCF • Longitude • Latitude • Radius of Earth • Angles (rad)
Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
2) Considerations for ARV Distribution • Spatial relation of HCF to neighbouring communities • ARV supply • Effective demand for each HCF • Longitude • Latitude
Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
3) Equity Objective Function • Purpose: find optimal equitable allocation strategy • Catchment region size • Number of HCF • Total number of ARV • Amount of ARV to each HCF • Precautions: • Total ARV supplied = Total ARV distributed • # ppl treated <= # HIV+ • + number of ARV to each HCP
… ugly math Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
Authors’ OEAS • Majority ARV to HCF in Durban • 2 non-Durban HCF have 5-15% • Other non-Durban HCF have <5% • When using current South Africa ARV roll out plan of 17 HCF
Comparison with other dist’n plans • Compare using fixed 40km catchment region • Ideal: 10% patients receive ARV at each HCF • Compare inter-quartile range: • 1) All ARV to Durban: • Small inter-quartile range; Unfair • 2) Equal ARV to 17 HCF: • Large inter-quartile range: 0.025-42% unequal access1) • 3) Authors’ OEAS: • Doesn’t necessarily deliver 10% to all patients • Small inter-quartile range 0.011 – 10% treated
Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
Comparison Con’t • Authors’ OEAS not perfect but gives best equality of ARV distribution
2) Catchment Region & # HCF • Equality improves SUBSTANTIALLY with either • # HCF used is more important than catchment size • 27 HCF1) 20km 88% 2) 40km 91%3) 60km 96% • 54 HCF1) 20km 90%2) 40km 94%3) 60km 99%
Photo source: Wilson DP, Blower SM (2005) Designing equitable antiretroviral allocation strategies in resource-constrained countries. PLOS Medicine. DOI: 10.1371/journal.pmed.0020050
2) Catchment Region & # HCF Con’t • Increase # HCF, SIGNIFICANTLY increase treatment accessibility • Propose: Increase in catchment region by increasing transportation
Best Strategy • Use all 54 HCF, each with catchment region of 40-60km to maximize ARV distribution
Suggestions for Improvements • Nigeria: Mobile clinic • Increase catchment region: • Challenge: improve transportation costly • Use all 54 HCF • Advantage: existing infrastructure • Challenge: training costly
Future Studies/Extensions • Data: distance patients willing/able to travel to HCF • Data: factor in travel ease for all communities • Different weighting function based on road infrastructure, availability of transportation etc.
Future Studies/Extensions Con’t • Authors chose equality as objective Other ethical ARV allocation strategies present • Need even access from national to grass root level • Proportion to province, HCF, groups of individual • If uneven access • Social, political structure destroyed • Intra-state, inter-state conflict
Patient Selection Reconsidered • 1) Behavioural core groups • Eg. sex workers • Challenge: fraud to receive priority treatment • 2) Highest viral load • Advantage: easy to identify • 3) Those s.t. reduce future epidemic impact • Advantage: potentially decrease future epidemic • Disadvantage: disregard current patients (unethical?)
Authors’ Conclusion • Our OEAS can be used by any resource-constrained country and highly recommended • Each nation has to decide on priorities of ARV distribution • Objective function can be modified but OEAS still apply
Personal Story • Movie Clip & Music!