Download
1 / 27
290 likes | 645 Views
PHARMACOKINETICS. 1. Fate of drugs in the body 1.1 absorption 1.2 distribution - volume of distribution 1.3 elimination - clearance. 2. The half-life and its uses. 3. Repeated administration of drugs. 4. Plasma concentration-effect relationship. 1. FATE OF DRUGS IN THE BODY.

E N D
PHARMACOKINETICS 1. Fate of drugs in the body 1.1 absorption 1.2 distribution - volume of distribution 1.3 elimination - clearance 2. The half-life and its uses 3. Repeated administration of drugs 4. Plasma concentration-effect relationship
1. FATE OF DRUGS IN THE BODY WHAT HAPPENS TO DRUGS INSIDE THE BODY Administered ABSORPTION Absorbed DISTRIBUTION „Hidden“ Volume of distribution Clearance Eliminated ELIMINATION Acting
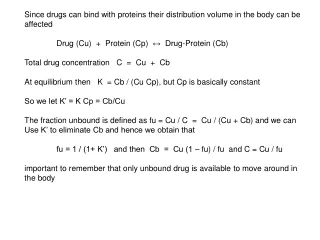
VOLUME OF DISTRIBUTION Depends on: • protein binding • plasma proteins • tissue proteins • ONLY A FREE DRUG ACTS! • The bound drug is inactive. • Free and bound drug are in equilibrium. • Displacement: drug-drug interactions
VOLUME OF DISTRIBUTION Vd = Amount of drug in body / Concentration of drug in plasma Because the result of the calculation may be a volume greater than that of the body, it is an APPARENT (imaginary, not actual) volume For example, Vd of digoxin is about 645 liters for a 70 kg man (i.e. about 9 times bigger that his actual volume)
Clinical importance of volume of distribution: • When Vd of a drug is big it takes long time to achieve effective plasma concentration of the drug. In such cases a loading dose may be given to boost the amount of drug in the body to the required level. This is followed by administration of lower maintenance dose.
CLEARANCE Clearance (CL) is the volume of plasma totally cleared of drug in unit of time (ml/min/kg) CLtot total CLR renal CLH hepatic CLNR nonrenal (= Cltot - CLR)
Clinical importance of clearance • Determines the maintenance dose • Drugs eliminated mainly through the kidney need measures (e.g. dosage adjustment) in renal insufficiency • Drugs eliminated mainly through the liver need protective measures in liver insufficiency
2. The half-life and its uses the half-life is the time taken for the plasma concentration to fall by half [plasmatic half-life]
In most drugs after therapeutic doses: plasma concentration falls exponentially Linear kinetics (First order) The rate of elimination is proportional to the concentration [t 1/2 is stable]
In most drugs after therapeutic doses: plasma concentration falls exponentially because elimination processes are not saturated Linear kinetics (First order) Cmax [some robustness to dose increase] Cmin Elimination is the bigger the higher is the level The rate of elimination is proportional to the concentration
Elimination processes are saturated e.g. in alcohol, after higher doses of phenytoin, theophyllin Non-linear (Zero-order, saturation) kinetics The rate of elimination is constant For example, in alcohol the rate of metabolism remains the same at about 1 g of alcohol for 10 kg of body weight per hour [unstable t 1/2 ]
In a few drugs at therapeutic doses or in poisoning, elimination processes are saturated Cmax [low robustness to dose increase] Cmin elimination is constant, limited Non-linear (Zero-order, saturation) kinetics
THE USES OF THE HALF-LIFE • T1/2 as a guide to asses: • 1/ At a single-dose: duration of drug action • 2/ During multiple dosing: • to asses whether a drug is accumulated in the body (it is - if the drug is given at intervals shorter than 1,4 half-lifes) and • when a steady state is attained (in 4-5 half-lifes) • 3/ After cessation of treatment: to asses the time taken for drug to be eliminated from the body (in 4-5 half-lifes)
[t1/2 = 1 - 2 h] Ampicillin - single dose
THE USES OF THE HALF-LIFE • T1/2 as a guide to asses: • 1/ At a single-dose: duration of drug action • 2/ During multiple dosing: • to asses whether a drug is accumulated in the body (it is - if the drug is given at intervals shorter than 1,4 half-lifes) and • when a steady state is attained (in 4-5 half-lifes) • 3/ After cessation of treatment: to asses the time taken for drug to be eliminated from the body (in 4-5 half-lifes)
„PRINCIPLE OF 4-5 HALF-LIFES“: If a drug is administered in intervals shorter than 1.4 half-life, then a steady state is attained after approximately 4-5 half-lifes This time is independent of dose. Steady state Plasma concentration t1/2
Why SS is attained after 4-5 half-lifes? Attainment of steady state (SS) during multiple dosing of drug at intervals of 1 half-life
THE USES OF THE HALF-LIFE • T1/2 as a guide to asses: • 1/ At a single-dose: duration of drug action • 2/ During multiple dosing: • to asses whether a drug is accumulated in the body (it is - if the drug is given at intervals shorter than 1,4 half-lifes) and • when a steady state is attained (in 4-5 half-lifes) • 3/ After cessation of treatment: to asses the time taken for drug to be eliminated from the body (in 4-5 half-lifes)
Elimination of a drug during 5 half-lifes of initial level % of total elimination
3. REPEATED ADMINISTRATION OF DRUGS STEADY STATE attained after 4-5 half-lifes • FLUCTUATIONS • proportional to dose intervals • blunted by slow absorption STEADY-STATE CONCENTRATIONS proportional to dose t1/2
Fluctuations of concentrations are the bigger the longer are intervals between administrations (of parts of total dose) Time (h)
Administration of parts of total dose at short intervals • produces smaller fluctuations of drug concentrations (levels) • an omission of a particular dose* does not need to cause an undesirable fall in drug concentrations (levels) *noncompliance
How to reduce fluctuations in drug concentrations? by administering: • The total dose in parts at short intervals – mostly inconvenient • Sustained-release preparations, infusions
Steady-state concentrations are proportional to dose Linear kinetics - diazepam toxic plasma concentrations daily therapeutic daily daily Time (days)
Non-linear, saturation kinetics - phenytoin plasma concentrations toxic daily daily therapeutic daily Time (days)
4. PLASMA CONCENTRATION - EFFECT RELATIONSHIP • Effects of drug • correlate with plasma concentrations • Therapeutic Drug Monitoring (TDM) • do notcorrelate with plasma concentrations • „hit and run“ • tolerance or sensitisation • active metabolites