Download
1 / 51
510 likes | 531 Views
Learn about the primary role of the inner ear in equilibrium, the importance of vestibular system, the anatomy of the labyrinth and otolith systems, and interesting studies related to hair cells and otoconia.

E N D
Why Vestibular testing Mohammad S Asghar
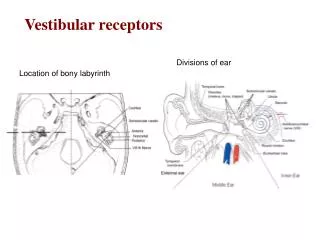
Primary role of Ear The primary role of the ear (the inner ear) is equilibrium. This statement is based on the phylogenic development of the inner ear. Phylogeny is the sequence of the embryological development of a species. The earlier in the development, the more primitive or necessary is its function. The labyrinth portion (vestibular) of the inner ear precedes the development of the cochlea.
Importance of Vestibular system Could a species survive hard of hearing or even deafness? Sure, but the species probably would have evolved making better use of its remaining sensory modalities; i.e. peripheral vision, etc. However, could a species survive without the ability to stand, coordinate eye and head movement, or navigate through space? No. The species obviously could not survive.
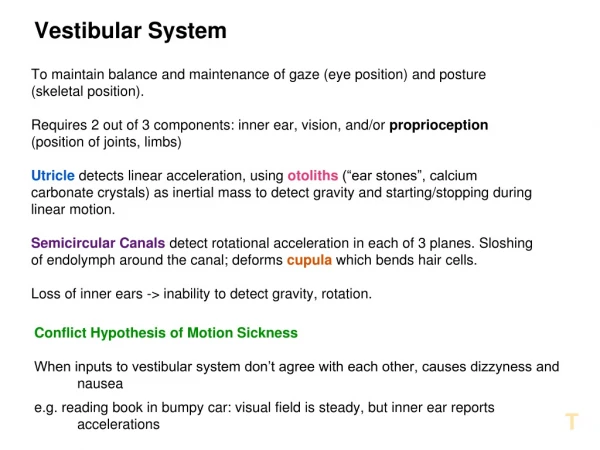
The two types of sensory receptors within the labyrinth are the semicircular canals (superior, horizontal and :posterior) and the Otolith mechanisms (utricle and saccule)
SSC Each semicircular canal is positioned and fine-tuned to be a velocity accelerometer in the plane in which it lays. At the base of each canal a widened area, the Ampulla, which houses tile sensory organ comprised of a cupula and cristae in which the nerve and hair cells are located.
Otolith system The Otolith Systems are gravitv detectors and provide information on acceleration in the horizontal and vertical Planes. The utricle lays horizontal and the saccule lays vertical. The sensory receptor nerve and hair cells are within the macula of each structure.
Anatomy conti Each labyrinth has two types of receptors with a total of five sensory organs. Each sensory organ almost resembles the cochlea’s organ of Corti, in that there is an area of nerve and hair cells and a gelatinous membrane(similar to the tectorial membrane) whose movement, caused by hydromechanical force, stimulates the hair cells’ cilia
The cupula within the ampulla of each semicircular canal is a gelatinous plug which sits atop the cristae. It is like the bristles of a toothbrush embedded in a movable plug of jello.
Anatomy conti The otoconia are Calcium carbonate crystals sitting atop the gelatinous plug above the otolith’s macula. The weight of the otoconia pressing on the cilia provide information on gravitational pull.
Anatomy conti Within the sensrny organs of semiclrcular canals, cristae and the otoliths macula are two distinct types of . hair cells. These are identical to the hair cell types found in 1he cochlea. Type I hair calls are often described as being “flask” shaped. Type II hair cells are cylindrical in shape.
Anatomy conti Type I hair cells sit within a chalice with only direct afferent nerve connection. The efferent connection is to the afferent nerve, not directly to the cell body. Type II hair cells have direct connections with afferent and efferent nerve endings called buttons. Afferent connections are ascending and excitatory and efferent connections are descending and inhibitory.
Anatomy conti Cilia: The cilia of the hair cells are similar to a light switch, in that they may become stimulated by their movement into either direction out of the neutral or resting state. Macula The sensory organ within the macula of the utricle and saccule have thousands of otoconia resting on the gelatinous layer above the cilia. .
Interesting study Recent publication by Merchant (1999 Laryngoscope) presented a breakthrough method of identifying and counting the hair cells, post mortum. For the first time, this study provided data on the difference in hair cells remaining in patients With a variety of vestibular disorders: Meniere’s patients were found to have the greatest loss in type II hair cells. With Type I cells relatively unaffected. Aminoglycide patients had a loss of both types.
Interesting study .1. How many cells must be lost before a vestibulopathy occurs, as measured by a caloric weakness? 2. Will the loss of one hair cell type vs. the other produce different test or functional fmdings1 3. Do various disorders affect hair cells differently? 4. Will the type of hair cell lost or remaining offer a different prognosis for compensation with and without VRT?
Otoconia The calcium carbonate otoconia are in a variety of shades and sizes. Is this the reason that some patients spontaneously clear their BPPV and others may have it linger for years? Is this the reason that some form of BPPV adheres to the cupula and another floats freely in the canal.
Blood supply BPPV is the leading cause of vertigo in persons over the age of 65. These are folks who have no prior otology history, i.e. Meniere’s or Vestibular neuritis (Meniere’s and vestibular neuritis patients do, however, have a higher incidence of BPPV than their cohorts). Is this because the utricle’s vascular supply is compromised, causing degeneration of the macula and releasing the “dead” otoconia to migrate? Anatomically, the posterior canal lays directly below the utricle. Although it has not been affected by decreased blood flow it becomes the wastebasket for the freed otoconia.
Anecdotally, 30-50% of patients with BPPV also have a vestibulopathy (caloric weakness) in that ear. Is this, too, a result of the slow vascular compromise of the anterior labyrinthine artery? Most likely it is.
Physiology of the system. Vestibular disorders are typically ablative or destructive.
Vertigo Vertigo is the hallucination of motion. [t derives from the French verb “yertere”, which means to turn. Vestibular disorders, which are slow, such as arteriosclerosis changes. Or slow growing tumors such as acoustic neuroma, may cause a vestibulopathy (caloric weakness) but without vertigo. This is most likely a result of compensation where the brain accommodates this asymmetry because it occurs over a long period of time.
Vertigo The hallucination of motion is heightened by the sensory conflict. While the vestibular systems message to the brain is that the head is turning quickly in one direction, the visual and somatosensory systems cannot corroborate that signal. So, vertigo could be described as the brain’s conscious reaction to sensory conflict.
The vestibular system is Stimulated by hydro mechanical~ changes caused by head movement. The movement or acceleration of the head to the right causes the endolymph fluid to move to the left. This pushes the cupula to the left, which bends the hair cells toward the Ampulla. This ampulopetal response is one of excitation. The vestibulo-ocular reflex then signals the extra ocular eye muscles to move the eyes in a compensatory manner to the left.
While this is happening in the ear of the side of the head that is accelerating, a second signal is coming from the opposite ear. This signal, however, is one of deceleration or inhibition, because the paired canals stimulation is ampulofugal, or away from the Ampulla.
Paired Comparisons: Right Horizontal – Left Horizontal Right Superior – Left Posterior Right Posterior – Left Superior
VOR The Vestibular-Ocular Reflex (VOR) allows for gaze stabilization during active head movement. The vestibular connections from the semicircular canals and Otolith mechanisms send information about head movement through the central pathways. Compensatory eye movements are created by innervations of the extraocular eye muscles.
VOR Because we are recording or observing the output portion of the VOR., abnormalities may he caused by labyrinthine, neurological or neuromuscular influences. The relationship of head and eye movement is measured as gain and phase. The VOR gain may be thought of as the strength of the eve movement. Simply stated, for every one degree of head movement there must be a corresponding one degree of eye movement (Gain = 1: 1 ). If there is not, there will be a loss of accuracy in the positioning of the eyes on the target.
VOR The phase component relates to the time relationship & of when the eyes have moved relative to the head .movement. The eye movement should be 180 degrees out of phase with the head movement. As normal head activity occurs between approximately .8 Hz – 6 Hz, it is actually the VOR that allows us to enjoy normal vision dung head movement. The visual system operates at a much slower rate and cannot focus without the VOR functioning properly.
A defect in either gain or phase may cause an oscillopsia. This may best be described as the inability to focus vision with head movement. It may occur with either horizontal or vertical head movement. This occurs due to the retinal slippage of an image as it cannot be positioned properly on the retina of the eye; It may be described by patients as things appear to be jumping off the page or a sense of motion sickness.
Many normal individuals cannot read in a car or follow a map while driving because of a normal but poorly “tuned” VOR function. Pursuit forms of eye movements are slow compared to the ability of the VOR to focus vision. During active and rapid head movement. These slow eye movement’s speed is limited by the neuromuscular capabilities of the extra-ocular eye muscles.
Pendular pursuit is a voluntary eye movement which allows tracking or smooth pursuit of a moving object with eyes only (head is stationary). Humans are capable of following moving object with eyes only up to speeds of about 4 HZ. An example of this type of eye movement might be as one does following a bird or airplanes flight through the sky.
Saccadic pursuit is also a voluntary eye movement. This calls for the rapid repositioning of the eyes between targets. This is similar to what one does while reading, moving the eyes from line to line.
Optokinetic pursuit is an involuntary visual response to movement. It is a combination of both pendular and saccadic pursuit. This is what occurs when perceiving, mostly through peripheral vision, the movement of traffic. The eyes will follow a car for a short distance (pendular), then rapidly reposition (saccade) to pick up the next one.
The neurological pathways of the pursuit system travel through the brainstem, cerebellum and the occipital-and parietal cortex. The vestibular systems central pathways are within the brainstem and cerebellum. This schematic graphic shows both the ascending and descending pathways.
Schematic of eye movement: Schematic of eye movement: Each cranial nerve has an influence on the patient’s ability to move their eyes. The majority of eye movement is controlled by CN III, the Oculomotor cranial nerve. Observing the patient’s ability to hold their eyes in an eccentric gaze (direct observation is okay, no equipment is needed) right, left, up and down can provide the examiner with a quick qualitative assessment of any neuromuscular dysfunction, i.e. ocular paresis.
VSR: The Vestibulo-Spinal Reflex is predominately a descending motor response pathway which Provides the musculoskeletal system through the reticulospinal tract with information for the anti gravity muscles. This provides information about posture and gravitational pull. This comes primarily from the Otolith mechanism.
Eye muscles. The eye is moved by six extra-ocular eye muscles. There are four Rectus muscles and two Oblique muscles. These six muscles are innervated by Cranial nerves Ill (Oculomotor), IV (Trochlear) and VI (Abducens). It is important to evaluate the eye movement capabilities of a patient, as virtually all vestibular tests record eye movement as an indirect measurement of peripheral and central vestibular function.
III Nerve: Supply, Medial, Inferior and superior rectus and also inferior oblique musceles. VI Nerve supply: Lateral rectus. IV Nerve supply: Superior oblique. Postural stability assessment and evaluation of compensating strategies, often provide both qualitative and quantitative patterns which correlate to specific abnormalities.
What is Vestibular Testing? Vestibular testing consists of a number of tests that help determine if there is something wrong with the vestibular (balance) portion of the inner ear. These tests can help isolate dizziness symptoms to a specific cause that can often be treated.
Why Get Vestibular Tests? If dizziness is not caused by the inner ear, it might be caused by the brain, by medical disorders such as low blood pressure, or by psychological problems such as anxiety. Recent studies have documented that vestibular tests are more accurate than clinical examination in identifying inner ear disorders (Gordon et al, 1996). Hearing pathway tests (audiometry, auditory brainstem response, electrocochleography) can also be used for the same purpose, and are frequently combined with vestibular tests.
Why Get Vestibular Tests? (conti) Vestibular tests can help determine if more expensive tests, such as magnetic resonance imaging (MRI), are needed. Recent studies (Levy and Arts, 1996) have shown that vestibular testing is much more accurate than clinical symptoms in predicting whether neuroimaging tests will be abnormal. Vestibular tests can also document objectively vestibular conditions such as benign paroxysmal positional vertigo (BPPV), and perilymph fistula, which commonly occur after head injury; and bilateral vestibular ototoxicity, which commonly is a side effect of medication.
Anatomical sites and causes of dizziness Central LSSC Brainstem Oculomotor Pathways Sup Vest Nerve ASSC MLF Vestibular Nuclei Oculomotor Nuclei Eye Movement Eye Muscle RF Utricle Inf. Vest Nerve PSSC Eyes(vision) Cerebellum Cerebral Cortex Saccule Spinal Cord Body Muscles Postural Movement Peripheral Vestibulospinal Pathways Vestibular tests Evaluate VOR, VCR & VSR There is no direct access to vestibular end organs
VEMP: literature Review (1994-2006)*