Download
1 / 40
570 likes | 1.23k Views
Ultrasonography. Dr. LeeAnn Pack Dipl. ACVR. Ultrasonography vs. Radiography. They complement each other Both have strengths and weaknesses Cost concerns correct selection All patients should receive abdominal radiographs before ultrasonography Get all the information

E N D
Ultrasonography Dr. LeeAnn Pack Dipl. ACVR
Ultrasonography vs. Radiography • They complement each other • Both have strengths and weaknesses • Cost concerns correct selection • All patients should receive abdominal radiographs before ultrasonography • Get all the information • May eliminate need for ultrasound
Strengths of Ultrasonography • Determining origin of an abdominal mass • Evaluation of organ parenchyma • Liver, spleen, kidneys, adrenals, pancreas, intestines, prostate, bladder, heart • Fetal viability • Real time scanning – see movement/motion • Performing fine needle aspiration/ biopsy • Cells or tissue NOT images ultimately give us the definitive diagnosis for neoplasia, etc. • Ultrasound does not provide a histopathologic diagnosis
Weaknesses of Ultrasonography • Ultrasound can’t penetrate gas or bone • Difficult to evaluate liver size, kidney size in dogs • Can’t assess intestinal gas patterns • Can’t evaluate some extra abdominal structures (i.e. spine) • Equipment can be expensive • Diagnostic success is user dependent • Must know anatomy very well
Why do you need both? • Examples • Prostatic adenocarcinoma seen on ultrasound • Has it spread to lumbar vertebrae? • Coughing patient with mitral regurgitation on echo • Does the patient have pulmonary edema? • Enlarged liver on radiographs • Can get a guided FNA with ultrasound
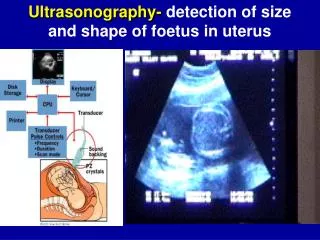
Basic Ultrasound Physics • Transducer (probe) • Piezoelectric crystal • Emit sound after electric charge applied • Sound reflected from patient • Returning echo is converted to electric signal- grayscale image on monitor • Echo may be reflected, transmitted, or refracted • Transmit 1% receive 99% of the time
Acoustic Impedance • The velocity of sound in a tissue and tissue density = determine acoustic impedance • Most soft tissues = 1400-1600m/sec • Bone = 4080, Air = 330 • Sound will not penetrate – gets reflected or absorbed • Travel time – dot depth
Attenuation • Absorption = energy is captured by the tissue then converted to heat • Reflection = occurs at interfaces between tissues of different acoustic properties • Scattering = beam hits irregular interface – beam gets scattered
Basic Ultrasound Physics • Sound waves are measured in Hertz (Hz) • Diagnostic ultrasound typically • 1-20 MHz • As frequency increases, resolution improves • As frequency increases, depth of penetration decreases Frequency Penetration
Examples of Ultrasound Probes A B C A B C
Transducers • Sector scanner – fan shaped beam • Small surface require for contact • Linear scanner – rectangle beam • Large contact area required • New ones are curvi-linear • These scan heads are much smaller with wide field of view
Basic Ultrasound Physics • Monitor and computer • Convert signal to an image/ archive • Tools for image manipulation • Gain – amplification of returning echoes • Overall brightness • Time gain compensation (curve) • Adjust brightness at different depths • Freeze • Depth • Zoom in superficial, or zoom out for wide view • Depth limited by frequency • Focal zone • Optimal resolution wherever focal zone is
Modes of Display • A mode • Spikes – where precise length and depth measurements are needed – ophtho • B mode (brightness) – used most often • 2 D reconstruction of the image slice • M mode – motion mode • Moving 1D image – cardiac mainly
Artifacts • Improper machine settings – gain • Reverberation • Mirror image – liver GB • Comet tail – gas bubble • Ring down – skin transducer surface • Acoustic shadowing • Acoustic enhancement • Edge enhancement • Border of kidney
Ultrasound Terminology • Never use dense, opaque, lucent • Anechoic • No returning echoes= black (acellular fluid) • Echogenic • Regarding fluid--some shade of grey d/t returning echoes • Relative terms • Comparison to normal echogenicity of the same organ or other structure • Hypoechoic, isoechoic, hyperechoic • Spleen should be hyperechoic to liver
Patient Positioning - Prep • Dorsal recumbency • Lateral recumbency • Standing • Clip hair • Be sure to check with owners • Apply ultrasound gel • Alcohol can be used – esp. in horses
Image Orientation and Labeling • Must be consistent • Symbol on screen ~ dot on transducer • “dot” to head and “dot” to patients right • “dot” lateral for transverse and proximal for longitudinal images • Label label label
Indications for Abdominal Ultrasonography • Same as with abdominal radiographs • Should have some idea of what you are looking for—not just a fishing expedition • Further investigate a radiographic finding • ***If clinical signs or history indicate abdominal ultrasound, then it should be performed even if radiographs are normal!!!
Ultrasound-guided FNA/ biopsies • NORMAL ABD U/S FINDINGS DO NOT MEAN ORGANS ARE NORMAL!!! • ***Do FNA if suspect disease • Abnormal u/s findings nonspecific • Benign and malignant masses identical • Bright liver may be secondary to Cushing’s dz or lymphoma • Aspirate abnormal structures (with few exceptions)!!! • Obtain owner approval prior to exam • Warn owner of risks • +/- Clotting profile
Ultrasound-guided FNA/ biopsies • Risks of FNA’s • Fatal hemorrhage • Pneumothorax w/ pulmonary masses • Seeding of tumors • TCC • Sepsis • Abscesses
Ultrasound-guided FNA/ biopsies • I Routinely aspirate • Liver (masses and diffuse disease) • Spleen (nodules and diffuse disease) • Gastrointestinal masses • Enlarged lymph nodes • Enlarged prostate • Pulmonary/ mediastinal masses (usually don’t biopsy due to risk of pneumothorax • I Occasionally aspirate • Kidneys (esp. if enlarged) • Pancreas • Urinary bladder masses • I Never aspirate • Adrenals • Gall bladder
Ultrasound-guided FNA/ Fine Needle biopsies • Non-aspiration Technique • 22g 1.5in needle • 6 cc syringe • Short jabs into organ • Spray onto slide, smear, and check abd for hemorrhage
Ultrasound-guided FNA • Aspiration technique • Same set up as with non-aspiration technique • With needle in structure, pull back plunger vigorously several times • Remove needle, fill syringe with air • Spray onto slide and smear
Ultrasound-guided Core Biopsies • Use a special biopsy “gun” • 14-20g • Insert thru small skin incision • Much more representative sample • Tissue not just cells • Sometimes it is necessary to get the answer • But…. MUCH MORE LIKELY TO BLEED!
Intro Summary • Know your limitations • Lack of expertise • $15,000 vs. $150,000 machine • For abd or thx, do radiographs first • If safe and reasonable, do FNA’s of all suspected abnormal structures based on history, clinical signs, or the ultrasound exam • Abnormal structures can look normal • Of the structures that do look abnormal, benign and malignant processes can be identical • Documentation – save images in some fashion