Download
1 / 2
40 likes | 470 Views
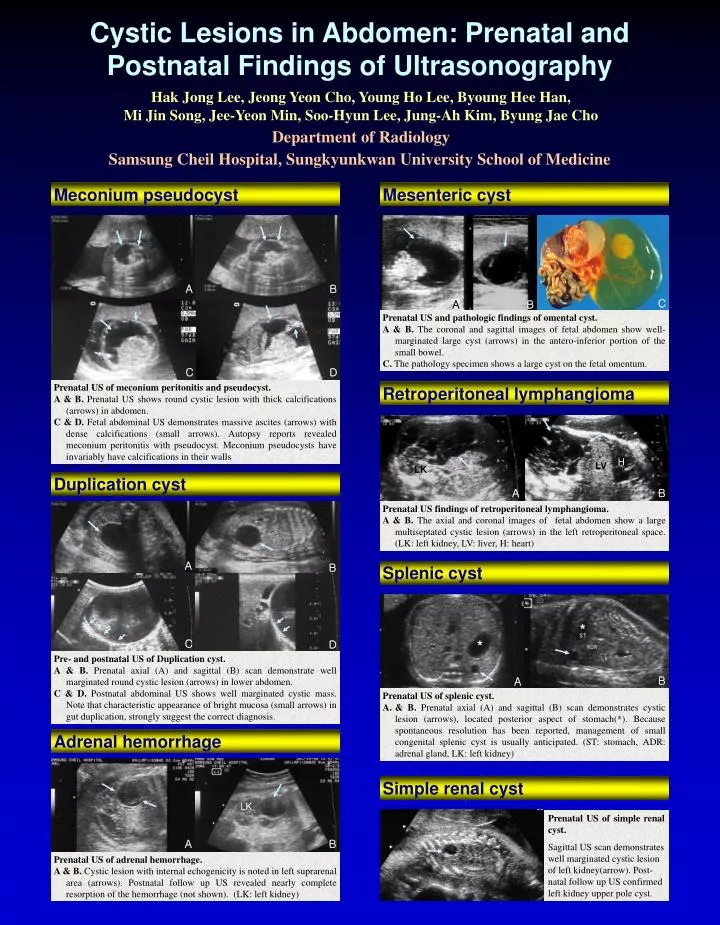
Cystic Lesions in Abdomen: Prenatal and Postnatal Findings of Ultrasonography. Hak Jong Lee, Jeong Yeon Cho, Young Ho Lee, Byoung Hee Han, Mi Jin Song, Jee-Yeon Min, Soo-Hyun Lee, Jung-Ah Kim, Byung Jae Cho. Department of Radiology

E N D
Cystic Lesions in Abdomen: Prenatal and Postnatal Findings of Ultrasonography Hak Jong Lee, Jeong Yeon Cho, Young Ho Lee, Byoung Hee Han, Mi Jin Song, Jee-Yeon Min, Soo-Hyun Lee, Jung-Ah Kim, Byung Jae Cho Department of Radiology Samsung Cheil Hospital, Sungkyunkwan University School of Medicine Meconium pseudocyst Mesenteric cyst A B C A B Prenatal US and pathologic findings of omental cyst. A & B. The coronal and sagittal images of fetal abdomen show well-marginated large cyst (arrows) in the antero-inferior portion of the small bowel. C. The pathology specimen shows a large cyst on the fetal omentum. C D Prenatal US of meconium peritonitis and pseudocyst. A & B. Prenatal US shows round cystic lesion with thick calcifications (arrows) in abdomen. C & D. Fetal abdominal US demonstrates massive ascites (arrows) with dense calcifications (small arrows). Autopsy reports revealed meconium peritonitis with pseudocyst. Meconium pseudocysts have invariably have calcifications in their walls Retroperitoneal lymphangioma H LV LK Duplication cyst A B Prenatal US findings of retroperitoneal lymphangioma. A & B. The axial and coronal images of fetal abdomen show a large multiseptated cystic lesion (arrows) in the left retroperitoneal space. (LK: left kidney, LV: liver, H: heart) A B Splenic cyst * * C D Pre- and postnatal US of Duplication cyst. A & B. Prenatal axial (A) and sagittal (B) scan demonstrate well marginated round cystic lesion (arrows) in lower abdomen. C & D. Postnatal abdominal US shows well marginated cystic mass. Note that characteristic appearance of bright mucosa (small arrows) in gut duplication, strongly suggest the correct diagnosis. B A • Prenatal US of splenic cyst. • & B. Prenatal axial (A) and sagittal (B) scan demonstrates cystic lesion (arrows), located posterior aspect of stomach(*). Because spontaneous resolution has been reported, management of small congenital splenic cyst is usually anticipated. (ST: stomach, ADR: adrenal gland, LK: left kidney) Adrenal hemorrhage Simple renal cyst LK Prenatal US of simple renal cyst. Sagittal US scan demonstrates well marginated cystic lesion of left kidney(arrow). Post-natal follow up US confirmed left kidney upper pole cyst. A B Prenatal US of adrenal hemorrhage. A & B. Cystic lesion with internal echogenicity is noted in left suprarenal area (arrows). Postnatal follow up US revealed nearly complete resorption of the hemorrhage (not shown). (LK: left kidney)
Simple hepatic cyst Cloacal dysgenesis A B A B Congenital hepatic cyst arising from aberrant intrahepatic ducts. A. Prenatal US shows ovoid shaped cystic lesion in right upper quadrant (arrows). This cystic lesion is located adjacent to gall bladder (small arrow), mistaken as choledochal cyst. B. Postnatal US shows that this cystic mass is surrounded by liver parenchyma (small arrows). Surgical resection was done with the impression of choledochal cyst, but the cyst was confirmed as simple hepatic cyst. C D Transvaginal US and autopsy specimen of cloacal dysgenesis. A & B. Transvaginal US reveals markedly dilated cystic structure (arrows), without evidence of vascular flow signal. C. Schematic drawings of cloacal dysgenesis. There is usually single opening on the perineum. This may result in obstruction of urine outflow with subsequent dilatation of urinary tract, genital and gastrointestinal tract. D. Autopsy specimen reveals markedly dilated cloaca (arrow). Choledochal cyst A B Bladder outlet obstruction Pre- and Postnatal US of choledochal cyst. A. Prenatal US shows relatively round cystic lesion with tubular structure (arrow), which is characteristic findings of choledochal cyst. B. Postnatal US shows similar findings of prenatal US. If tubular structure (arrows) can be identified either entering or leaving a right upper quadrant cyst, the diagnosis of a choledochal cyst is ensured. This case was confirmed as choledochal cyst after surgery. A B C Multicystic dysplastic kidney Transvaginal US of 13 weeks fetus showing bladder outlet obstruction. A & B. Markedly dilated bladder (arrows) is noted on transvaginal US. C. Autopsy specimen revealed markedly dilated urinary bladder (arrow). Ovarian cyst A B US and pathologic specimen of MCDK. A. Prenatal US shows multiple dilated cystic lesions (arrows) in the left renal fossa. B. Pathologic specimen revealed multiple cystic mass of left kidney confirming multicystic dysplastic kidney. BL A B C Prenatal (3.3 cm) 1 wk (2.1cm) 5wks (1.5cm) Serial changes of ovarian cyst in prenatal and postnatal US. A. Prenatal US demonstrates large cystic mass (arrow) located in right, superior aspect of bladder. The gender of the fetus was female. B & C. Serial follow up US scans one week (B), and 5 weeks (C) after birth show gradual decrease of the cyst size (arrows). (BL: urinary bladder) UPJ obstruction References • Hill LM. Ultrasound of Fetal Gastrointestinal Tract. (In) Callen PW. Ultrasonography in Obstetrics and Gynecology, 4th ed. 2000: 457-488. • Sato M, et al. Mesenteric cyst: sonographic findings. Abdom Imaging 2000; 25(3): 306-310. • Barr LL, et al. Enteric duplications in children: are their ultrasonographic wall characteristics diagnostic? Pediatr Radiol 1990;20(5): 326-8. • Ros PR, et al. Mesenteric and omental cysts: histologic classification with imaging correlation. Radiology 1987;164(2): 327-32. • Teele RL, et al. The abdominal mass in the neonate. Semin Roentgenol. 1988 Jul: 23(3): 175-84. • Katsohis CD, et al. Retroperitoneal mesenteric cysts. Int Surg. 1989; 74(1):28-31. A B Prenatal US of hydronephrosis due to ureteropelvic junction obstruction. A. Prenatal US shows marked dilated pelvocalyceal system (arrows). In some instances, markedly dilated pelvocalyceal system can mimic abdominal cystic mass. Note that multicystic lesions (small arrows) of contralateral kidney, confirmed to be MCDK. B. Oblique coronal scan demonstrates that this cystic mass is dilatation of pelvocalyceal system.