Download
1 / 46
460 likes | 533 Views
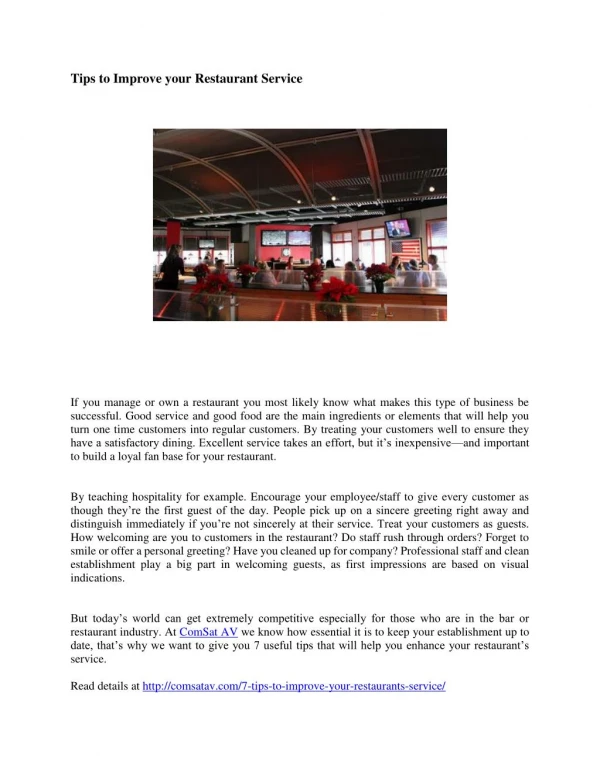
How to Improve ACTT Practices Based on Criticism. Wendy Chow, MSW RSW Assistant Professor, Dept of Psychiatry, University of Toronto Head, International Education, Dept. of Psychiatry, University of Toronto

E N D
How to Improve ACTT Practices Based on Criticism Wendy Chow, MSW RSW Assistant Professor, Dept of Psychiatry, University of Toronto Head, International Education, Dept. of Psychiatry, University of Toronto Program Manager, Assertive Community Treatment and Mental Health Court Support ProgramVice President, Ontario ACT Association Dr. Joel Sadavoy, M.D., F.R.C.P (C) Professor and San and Judy Pencer and Family Chair in Applied General Psychiatry, University of Toronto Director, the Cyril and Dorothy, Joel and Jill Reitman Centre for Alzheimer Support and Training Head Geriatric and Community Psychiatry Program, Mount Sinai Hospital Ontario ACT Association 2012 Workshop April 19-20, 2012
Outline • Who are the clients treated in ACT? • Addressing clients criticisms of ACT • Intervention & techniques to form better therapeutic relationships
Schizophrenia is a complex illness. • Integrated medication, psychosocial and rehabilitative approaches are necessary for effective treatment (APA guidelines for Rx of patients with Schiz 1997)
The Perfect System • Based on thenature of the disease/dysfunction rather than traditional institutional organizations • Integrates the full array of necessary services- social and medical • Addresses thesocial breakdownin families, work, friendships, physical health needs etc • Addresses the inevitable need for intermittentacute institutional care
Schizophrenia is not a hopeless disease but takes special skills to manage it • 1/3 do well over time • 1/3 do moderately well (i.e. stabilized even though symptomatic) • 1/3 do poorly with relapses and poorly controlled symptoms- they never really get better (these are the clients usually treated by ACT teams) (Wahlbeck et al Cochrane Database of systematic reviews, 3, 2003)
Factors in Poor Outcome Group • Inherent nature of the disease • Treatment failures- medication non-compliance; medication is essential • Client’s Isolation, homelessness, family/social rejection, unemployment, and loss of sense of self • Under treated medical illness, especially culturally diverse populations • MH systems are not well structured to deal with this problem.
ACT Studies • ACT extensively studied in RCT’s • Reduced hospitaluse in 74% of studies (eg. McGrew et al 1995, Tibbo et al 1999,Lehman et al 1997 ) • Housing stability-67% of studies • E.g.. Reduces homelessness – (Lehman et al 1997) • Improved QOLin 58% • Very good client satisfactionin 88% of studies
One yr/6month Reduction in IP Hospitalization After Admission MSHACT/ KACTT
Reduction in Inpatient Hospitalization After Admission into Mount Sinai Hospital Assertive Community Treatment TeamThree Year Follow Up Study ( n=61)
Client Criticisms of ACT (1) • Very Little literature on satisfaction McGrew J., Wilson R, Bond G. An Exploratory Study of What Clients Like Least About Assertive Community Treatment Psychiatry Serv 2002; 53:761-763
Client Criticisms about ACT (2) • McGrew et al 2002 • N=182 • Results : • No complaints - 44% • Home visits, intrusiveness, overemphasis of medications- 21% • Service frequency, availability of staff - 16% • Insufficient financial support, inconvenient location of program - 19%.
What are the reasons clients resistant to medication? • Medication sometimes does not work • Side effects lead to impaired function and self perception • Poor alliance with and trust of team/clinicians and mental health workers impairs compliance • Medication experienced as stigma, external control, symbol of failure • Failure to develop a concept of medication as an ally
Medication is essential to good outcome • High relapse group-one year relapse rates in responsive clients: 45-70% with placebo, 20- 30% with typical antipsychotic (atypical may be a little better) • Medication maintenanceappears essential (although not sufficient on its own) (e.g. Tran et al 1998; Ohmori et al 1999 Deliva et al 1998; Carpenter 1996) • 2.5-10 fold decrease in relapse rate with medication (Davis 1985)
Clients Criticisms of ACT Frequency of contact
Recommend minimum of 2/week Flexibility is essential and tailored to needs of the client and symptoms
Clients Criticisms of ACT Availability of Staff
Availability of Staff 24/7 model has many challenges: e.g. staff willingness, funding, burnout; team management is essential in this model
Clients Criticisms of ACT Location
ACT program offices need to be close to clients in the community But the office is not the primary location of service provision; overemphasis on office management defeats ACT model
Clients Criticisms of ACT Intrusiveness
Intrusiveness emerges when there is poor alliance with the client and failure to allow maximum autonomy based on functional capacity
Six important elements to reduce sense of intrusiveness • Empathyas the core of the alliance • Uncover the person within the illness • Understandthe Trauma of illness • Learn the client’sinternal experience of their illness • Understand theimpact of chronic illness • Understand client’sself perception as it relates to Medication-Compliance and attitudes to medication
Evidence for the Importance of the Psychological Perspective • Clinical - Clients tell us: what they experience as positive and negative in therapy • Frequent failure to establish an empathic alliance • Desire to avoid treating this population- frequent relapse and little improvement (Parker et al) • Failure to establish empathy is related to high staff/clinician and mental health worker burnout rates (Astroem et al) • Evidence for psychotherapeutic efficacy • Adjunctive therapy in combination with medication (Meuser) • Effectiveness of CBT (Tarrier et al, Sensky et al)
Regardless of presentation the Psychological therapeutic tasks remain the same • Establish relationship and therapeutic alliance to the greatest extent possible- engage with the healthy remaining part • Client almost always has double bookkeeping • Develop a psychological understanding of the client • Based on the idea that the client’s illness occurs in an inner psychological context that interacts with the outside world • Clinicians and mental health workers’ task is to understand this context and use it for the client’s welfare
Empathy • The degree to which an individual can mentally identify with another and see ( and feel ) the world as they do. Trial identifications while attempting to understand • Much more challenging with experiences that are highly unusual or repugnant eg. Hallucinations or delusions • May be enhanced by a shared group experience among clinicians and mental health workers
Uncovering the person within the illness: Who is the client? • Client often feels like a diagnosis not a person • The illness exists in the context of the client’s life and development • The client’s psychic reality • Dreams, ambitions, loneliness, isolation, rejection, hopelessness, self-perceptions • Sources of happiness and creativity • Cognitive distortions about the illness and its treatment
Internal Experience 1 • Cognitive Distortions • I am incurable • I am shameful • Others cannot love or care about me • My drugs are dangerous/will harm me • Nobody understands/believes me • People think I am crazy/bad/dangerous symptoms
Internal Experience 2 • Impact of hallucinations on function and concentration • Experience of delusions • Not being believed/labeled crazy • Fear and panic • Desire • Grandiosity • Responsible for bad events
Trauma of the Illness • Emergency/police/hospitalization experiences- force and compulsion • Medication side effects- contribute to negative symptoms • Societal reactions/ violence/ living on the street • Family rejection • Harsh clinicians and mental health workers
Chronicity • Chronic maladaptive beliefs and patterns of interaction with others • Chronic impaired or maladaptive social interactions- friendships within the “misfit” community • Substance abuse • Inadequate living/economic arrangements • Fears - eg. Robbery, violence, illness • Chronic illnesses- inadequate medical care
Medication and Self perception • Compliance related to alliance with clinicians, mental health workers and trust • Mistrust of the system - authorities and health workers reinforced by paranoid thought patterns • Negative side effects lead to impaired self perception and function • Medication as visible stigma • Medication as symbol of external control • Medication as symbol of failure • Developing a concept of medication as an ally
Goals and Tasks of Psychological Intervention 1 • Engaging the client and connecting with them • Understanding and therapeutic relationship/alliance • Translating behavior into meaning • Communicating- finding a common language • Destigmatizing • Dealing with shame, loss, identity, relationships and sexuality • Setting realistic goals
Goals and Tasks of Psychological Intervention 2 • Maintaining a therapeutic stance - limit setting • The holding environment - containment/reducing alienation/therapeutic haven • Tolerating uncertainty confusion, not knowing and sometimes anxiety or fear • Hopelessness/nihilism- the client cannot form a therapeutic alliance at first; suicide ( 50 times higher in Scf ) • Managing Therapeutic isolation • Frustration - transference and how not to take it personally
Creating and Sustaining a Relationship Factors • “Know” the client • Establishing trust (uncertain course and vicissitudes) • Persistence and re-finding the relationship • Fluctuations in the relationship • Boundary issues • Managing one’s own feelings • Guilt, anger, anxiety, tension, fear, confusion, tolerate ambiguity (to know and not know at the same time) • How not to take it personally • The hopeless therapist/ clinicians/ and mental health workers
Knowing the client: what does this mean? • Ask about their life and create a narrative • Inquire about the client in a manner that creates an emotional understanding- not just facts
The Role of History and Developmental Factors • Early life experience- family dynamics • Effects of adult life experiences including culture and immigration • Traumatic events • Character and personality evolve over time
Techniques 1 Creating a safe space • No physical contact • Absolute confidentiality, but within the team structure • Non-judgmental • Reliable - I do what I say • Containing client • Consistent - regularity and predictability of contacts • Available - personal vs. team • Don’t retaliate or withdraw- deal with own feelings without them coming out in the therapy- client takes advantage of you or client who seems to take advantage of you (client is 2 hours late and you are really busy and then they are mad at you) - how not to take it personally • Inquiring and seek to understand
Techniques 2 • Creating an alliance means determining what part of the client remains healthy ie. Is there a part of the client that remains intact and capable of insight or understanding • Some healthier parts almost always present to some degree
Techniques 3 Explore clients experience of their illness - convey to client your desire to understand • Impact of illness on their relationships • Impact of illness on their self esteem • Practical effects- job, money living situation • Effect on family and acceptance by society
Techniques 4 • Understand the client first from their own perspective without imposing your own at first • How do they see their situation, the causes of their illness, the best treatments • Collaborate instead of confrontation
Techniques 5 • Set mutually agreed on goals to the extent possible • Goals should be practical and realistic • Sometimes necessary for the clinicians and mental health workers to set limits • Non-judgmental and not angry limits - ie non-punitive limit setting
Techniques 6 • The process does not go in a straight line- ups and down • Recognize and tolerate client’s need for elements of control
Techniques 7 • Ambivalence- inherent in the illness • Thought disorder- unusual associations; learn clients mode of communication and use of language, distortions and symbolism • Look for subtle clues to what the client is experiencing when his affect is inappropriate- eg. laughter when anxious or sad • Understand client’s need for distance and nature of unusual emotional expression • Attend to what triggers hallucinations • All this emerges in the course of the therapeutic encounter
Techniques 8 • Group Activities • Life skills group • Line dancing group • Music group • Baking group • Noodle group • Groups address the needs of our clients
References • Tarrier N et al randomized controlled trial of intensive cognitive behavioural therapy for patients with chronic schizophrenia BMJ 1998;317:303-307 • Sensky T et al A randomized controlled trial of cognitive-behavioral therapy for persistent symptoms in schizophrenia resistant to medication Arch Gen Psychiatry 2000;57:165-172 • Packer S et al Psychiatric residents’ attitudes toward patients with chronic mental illness Hosp Comm Psychiatry 1994;45:1117-1121 • Woodside H et al Hope and Schizophrenia: exploring attitudes of clinicians Psychosoc rehab J 1994;18:140144 • Astroem S et al Staff burnout in dementia care: Relations to empathy and attitude Int j Nursing Studies 1991;28:65-75 • Fox V. Empathy : the wonder quality of mental health treatment Psychiatric rehab J 2000;23:292-293 • Meuser K et al Psychosocial treatment approaches for schizophrenia Curr Opinion in Psychiatry2000;13:27-35