Download
1 / 18
190 likes | 370 Views
Assessment of Efficacy and Safety for Exanta (Ximelagatran). Ruyi He, M.D. Medical Team Leader The Division of Gastrointestinal and Coagulation Drug Products September 10, 2004. Advisory Committee Meeting September 10, 2004. Outline. Short-Term Use

E N D
Assessment of Efficacy and Safety for Exanta (Ximelagatran) Ruyi He, M.D. Medical Team Leader The Division of Gastrointestinal and Coagulation Drug Products September 10, 2004 Advisory Committee Meeting September 10, 2004
Outline Short-Term Use Exanta 36 mg bid for 7-12 d (mean 8 d) : total knee replacement surgery (TKR) Efficacy: asymptomatic distal DVT Safety: bleeding, liver toxicity, MI/CAD Long-Term Use Exanta 24 mg bid for 18 months : VTE-P Exanta 36 mg bid for > 12 months (mean 16 m): AF Efficacy: non-inferiority margin in AF trials Safety: liver toxicity, withdrawal and MI/CAD
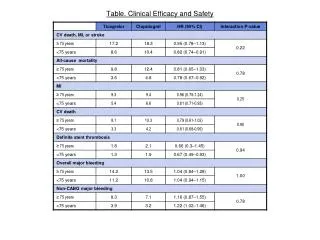
Efficacy: Short-Term Use in TKR Exanta was significantly better than Warfarin for primary endpoint: the incidence of total VTE and/or all-cause mortality (21.7% in Exanta group, 30.2% in Warfarin group, p<0.001). • There are no appreciable differences between groups for symptomatic DVT, proximal DVT, PE or death. • Efficacy result on Exanta is driven by decrease in asymptomatic distal DVT which is not clinically meaningful.
Short-Term Use: Liver Toxicity Number of patients with ALAT >3x ULN on treatment (OT) or follow-up (F/U) period__________ ______________________________________Exult A + B Exanta 36 mg Warfarin____________________________ ___________________OT (7-12 d) 13/1818 (0.72%) 18/1791 (1.0%) 4-6 w F/U 7/1784 (0.4%) 1/1776 (0.05) ________________________________________________ No fatal or non-fatal liver SAEs during OT and 4-6 w F/U period.Summarized from Table SP 42.
Short-Term Use: MI/CAD Adverse Events *Statistically significant in a post-hoc analysis @ one sudden death (ID#:15016) in W group is included as MI and 2 sudden deaths (ID#: 14366 and 12122) in X group are excluded from the analysis. Noted: 4 cases who did not take study drugs were excluded from this analysis (3 in X group: # 3206, 7086, 10944 and 1 in w group: # 9089). Summarized from Module 5, Table 54, Table 11.3.5.1 and Table 11.3.5.2
Short-Term Use: Summary of Safety Concerns for Exanta 2-fold higher incidence of major bleeding events ~3-fold higher incidence of acute MI/CAD. • Potential for duration of treatment to be > 12 d in clinical practice. • Higher incidence of ALT >3x ULN during 4-6 w F/U period, and no long-term (> 4-6 w) F/U data.
Long-term use: Efficacy in AF Sponsor’s pre-specified 2% non-inferiority margin too liberal SPORTIF III & V produced divergent results • Based on the double-blind, SPORTIF V study, it could not be ruled out that the risk of stroke/SEE was 2-fold greater on Exanta compared to Warfarin (95% CI = (0.91, 2.12))
Long-Term Use: Liver Toxicity Studies excluded patients with: Known clinically significant liver disease Persistent ASAT and/or ALAT >2-3x ULN Continuous treatment with NSAID or Known drug addiction and/or alcohol abuse Before 11/01(60%) LFTs monthly x 6; if ALAT >3x ULN, then weekly; if >7x ULN, Exanta was stopped. After 11/01(40%) LFTs monthly x 6; if ALAT >2x ULN, then weekly; if >5x ULN or >3x ULN for 4-8 w, Exanta was stopped.
Liver Toxicity (continued) ________________________________________________________ Exanta Comparators n=6948 n= 6230 _______________________________________________________ ALT >3x ULN 546 (7.8%) 74 (1.1%) ALT >3x ULN + 37 (0.53%)** 5 (0.08%) Bili. >2x ULN* ________________________________________________________ * Severe liver injury with mortality of 10 to 50% (Hy’s Law) ** 9 of 37 died. 3 deaths may have been related to Exanta. ITT population.
Case 1 (#7259): 80 y, M, on Exanta 36 mg bid for AF Day Event 1 ALT: 16 30 ALT: Normal 56 ALT: 2x ULN 85 ALT: 20x ULN (970). Exanta discontinuation 100 ALT: 30x ULN (1502), T. Bili. 2.4 108 Liver Biopsy: acute submassive necrosis 114 INR: 1.7, Alb: 2.9, T. Bili: 10.7, PT: 16.3, 119 INR: 1.8, Alb: 2.5, T. Bili: 17.1 145 Died GI bleeding with coagulopathy Autopsy: a small, friable and diffusely mottled liver with extensive liver necrosis, hepatocyte dropout and bile duct proliferation.
Case 2 (#7859): 77y M on Exanta 36 mg bid for AF Day Event 1 LFT: normal, Alb: 3.6 30 LFT: normal 63 ALT: 216 (4.5x ULN), T. Bili: 1.3 67 Weekly test, result unknown 81 Bloody stools, BP: 76/45, Hb: 7, PT: 37, aPTT: 69, INR: 3.4, plasma melagatran: 0.25 M (therapeutic range) ALT: 569, Alb: 2.0, pRBC 19U, FF plasma 15U, cryoprecipitate 30U, vit. K and fluids. 82 T. Bili: 10.4 (D. Bili: 5.2), gastroscopy: active bleeding, more pRBC, FFP, platelets and fluids, died from GI bleeding with profound coagulopathy. No autopsy.
Case 3 (#5442): 73y, M on Exanta 36 mg bid for DVT Day Event 1 ALT: 1.9x ULN 12 ALT: 4.5x ULN 18 ALT: 7.8x ULN, Hepatitis B diagnosed 22 ALT: 367, T. Bili: 1.8 24 Exanta discontinuation 26 ALT: 518, T. Bili: 4, INR: 2.3 42 ALT: 189, T. Bili: 26.8, hepatic encephalopathy 44 Died from liver failure
Long-Term Exposure: Discontinuation of Study Drug due to an Adverse Event (DAE) __________________________________________________________________________________________ AE Exanta comparators n=6931 n=6216_____________________________________________________________________________________________________________Total DAE 1189 (17.2) 801 (12.9)LFT abnormal 319 (4.6) 18 (0.3)MI/CAD 196 (2.8) 121 (1.9)Bleeding 83 (1.2) 43 (0.7)Cerebrovasc. Disorder 70 (1.0) 57 (0.9)DVT/PE 44 (0.6) 116 (1.8)*____________________________________________________________________*Placebo controlSummarized from sponsor’s Table NP 53long-term exposure safety population
Long-Term Exposure: Summary of Safety Concerns for Exanta • Higher incidence (0.53%) of severe liver injury (ALT >3x ULN + T. Bili. >2x ULN), including 3 deaths despite protocol specified LFT monitoring scheme. • In VTE population, higher incidence of acute MI/CAD with Exanta, including in placebo control study. • Higher incidence of withdrawal due to AE, including acute MI/CAD and bleeding events.
Acknowledgments All members of the Exanta Review Team Especially Dionne Price, Ph.D., Division of Biometrics II Suliman Al-Fayoumi, Ph.D., Division of Biopharmaceutics I Maria Ysern, M.Sc. Division of New Drug Chemistry II Mehul Desai, M.D., Divison of Cardio-Renal Drug Products John Lawrence, Ph.D., Divison of Biometrics I Alice Kacuba, RN, MSN, RAC, Regulatory Project Manager Ke Zhang, Ph.D, Division of Gastrointestinal and Coagulation Drug Products