Download
1 / 28

E N D
1. Clinical Evaluation of RanolazineEfficacy and Safety Andrew A. Wolff, MD, FACC
Sr VP, Clinical Research and Development
CV Therapeutics, Inc.
2. CE-2 Demonstrated in 5 double-blind, randomized, placebo-controlled studies
Dose and plasma concentration dependent
Observed in a broad population with severe coronary disease
Not dependent upon decreases in blood pressure or heart rate
At least as great as atenolol 100 mg qd
In patients on atenolol or diltiazem at doses considered optimal by their physicians
3. CE-3 Studies Demonstrating Efficacy of Ranolazine Two pivotal Phase 3 studies of ranolazine SR
MARISA: monotherapy, 191 randomized
CARISA: combination, 823 randomized
1� efficacy variable: trough exercise duration
Three supportive studies of ranolazine IR
4. CE-4 MARISA and CARISA Enrolled a Broad Population of Chronic Angina Patients
5. CE-5 Baseline Duke Score at Trough�All Randomized PatientsMARISA (CVT 3031) and CARISA (CVT 3033) Is Rand stand for All Randomized Patients?Is Rand stand for All Randomized Patients?
6. CE-6 Monotherapy Assessment of Ranolazine In Stable AnginaMARISA (CVT 3031) Patients withdrawn from other anti-anginals(N = 191 randomized)
Randomized, double-blind, 4-period crossover
1-wk treatment periods
Placebo vs 500, 1000, and 1500 mg bid
Exercise tests after each week of treatment
At trough (12 hr after dosing)
At peak (4 hr after dosing)
7. CE-7 Monotherapy With Ranolazine Increases Exercise Performance at Trough and Peak MARISA (CVT 3031)
8. CE-8 Combination Assessment of Ranolazine In Stable AnginaCARISA (CVT 3033) Randomization criteria identical to MARISA except for background therapy
Atenolol 50 mg qd (n = 354), or
Amlodipine 5 mg qd (n = 256), or
Diltiazem CD 180 mg qd (n = 213)
Three parallel groups for 12 wk of treatment
Placebo
Ranolazine 750 mg bid
Ranolazine 1000 mg bid
Exercise testing
At trough after 2, 6, and 12 wk of treatment
At peak after 2 and 12 wk of treatment
9. CE-9 Ranolazine With a Beta- or Calcium Blocker Increases Exercise Times at Trough and Peak CARISA (CVT 3033)
10. CE-10 Ranolazine Decreases Weekly Angina Attacks and Nitroglycerin ConsumptionCARISA (CVT 3033)
11. CE-11 Ranolazine SR Dose Predicts Concentration Combined Data From MARISA and CARISA
12. CE-12 Ranolazine Concentration Predicts ResponseAcross the Chronic Angina Population�Population-Based Analysis of Exercise Duration Four double-blind, placebo-controlled studies
MARISA, CARISA and 2 IR studies
1397 patients (1073 men, 324 women)
10,998 ETT-plasma concentration pairs
No influence on concentration-response
Demographic factors: age, weight, and race
Concurrent diseases: CHF class, diabetes
Background anti-anginal therapy
Men and women respond differently
Women: 6.4 sec/1000 ng/mL, 95% CI (3.1, 9.7)
Men: 16.8 sec/1000 ng/mL, 95% CI (14.6, 19.0)
13. CE-13 Anti-Anginal Effects of Ranolazine SR in Women Significant increase in exercise duration
6.4 sec per 1000 ng/mL, 95% CI (3.1, 9.7)
14. CE-14 Exercise Duration by Subgroup�Borderline Vital Signs or AV Conduction�MARISA (CVT 3031) and CARISA (CVT 3033)
15. CE-15 Ranolazine Is Effective Across a Broad Spectrum of Chronic Angina PatientsSubgroups Often Intolerant of Other Anti-Anginals Subgroups in which the effect of ranolazine appears consistent with the effect demonstrated in all patients:
Borderline vital signs or AV conduction�
Reactive airway disease
Congestive heart failure
Diabetes
16. CE-16 Ranolazine Is at Least as Effective as Atenolol 100 mg DailyRAN080
17. CE-17 Different Anti-Anginal Pharmacodynamics of Ranolazine vs AtenololEffects on RPP in RAN080
18. CE-18 Ranolazine With Atenolol or DiltiazemRAN072 �� patients � receiving an optimal dose of � beta blocker or diltiazem and stabilised at this optimal regimen for at least 7 days.�
2-period, double-blind, crossover design
Exercise tests 2.5 to 3 hr after dosing
Both ranolazine and background Rx at peak
Efficacy with 240 mg IR single dose (N = 25)
15 on atenolol (90 � 21 mg qd)
10 on diltiazem (186 � 19 mg qd)
19. CE-19 Exercise Performance 3 hr After Single Dose of Ranolazine 240 mg With Atenolol or DiltiazemRAN072
20. CE-20 Summary�Anti-Anginal and Anti-Ischemic Efficacy of Ranolazine Dose and plasma concentration dependent
Consistent throughout a broad population of chronic angina patients
Not dependent on decreases in blood pressure or heart rate
At least as great as atenolol 100 mg qd (RAN080)
In patients on atenolol or diltiazem at doses considered optimal by their physicians (RAN072)
21. Ranolazine Safety
22. CE-22 Safety of Ranolazine Extent of exposure
2783 subjects/patients
1714 subject/patient yr
Adverse events are generally dose dependent and manageable by typical dose titration
No evidence for an adverse effect of ranolazine on survival
23. CE-23 Extent of Ranolazine Exposure
24. CE-24 Duration of Exposure� 1714 subject/patient yr
1275 angina patient yr on SR
Mean exposure of angina patients to SR = 495 days
850 for > 30 days
503 for > 1 yr
259 for > 2 yr
25. CE-25 Ranolazine Was Well ToleratedAdverse Events Reported in = 2% of Patients and More Frequently on Ranolazine Than on Placebo
26. CE-26 Incidence per Patient Yr of Death and Sudden Death
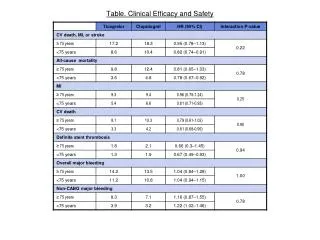
27. CE-27 Mortality in Controlled Studies
28. CE-28 Summary� Ranolazine Efficacy and Safety Efficacy demonstrated in 5 double-blind, randomized, placebo-controlled trials
Safe and well tolerated
Adverse events are generally dose dependent and manageable by typical dose titration
No evidence for an adverse effect of ranolazine on survival