Download
1 / 52
520 likes | 728 Views
GASTROINTESTINAL SYSTEM AND SLEEP. Oya İtil DE Medical Faculty Dept. Of Respiratory Medicine İZMİR. Sleep Disorders and GIS Symptoms. Disturbed sleep is common among patients with GI symptoms. Chicken, egg or vicious cycle ? Sleep disturbance is commonly reported by GER sufferers.

E N D
GASTROINTESTINAL SYSTEMANDSLEEP Oya İtil DE Medical Faculty Dept. Of Respiratory Medicine İZMİR
Sleep Disorders and GIS Symptoms • Disturbed sleep is common among patients with GI symptoms. • Chicken, egg or vicious cycle ? • Sleep disturbance is commonly reported by GER sufferers.
There is an association between irritable bowel syndrome and sleep disorders. • Waking up at least four times a month has been found to be associated with a variety of GI symptoms like pain and diarrhea.
Sleep disorders can lead to changes in visceral sensations. • Sleep deprivation hyperalgesia M. Maneerattanaporn. Neurogastroenterol Motil 2009;21:97-99
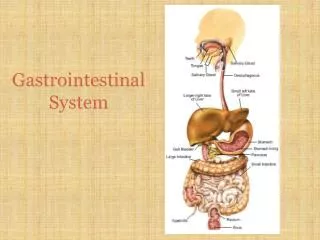
GER Passive transition of gastric content into the oesophageus due to the transient or chronic relaxation of lower oesophageal sphincter
Retrosternal burning sensation and / or pain • Regurgitation of gastric content • Bitter taste in mouth • erozive oesophagitis ( stricture, Barrett metaplasia, adenocarcinoma ) • May be asymptomatic
Nonerosive form 60 % • Erosive form 35 % • Complicated erosive cases 5 %
Pulmonary Asthma Aspirationpneumonia Chronic bronchitis Pulmonary fibrosis Cardiac Chest pain ENT Hoarsness Laryngitis Pharyngitis Chroniccough Globus sensation Disphonia Sinusitis Subglottic stenosis Laryngeal cancer Extraoesophageal Manifestatıons of GER
GER- related oral andlaryngopharyngeal manifestations • Larynx oedema and hyperemia • Vocal corderythema, polyps, granulomas, ulcers • Hyperemia of posteriorpharynx and lymphoid hyperplasia • Interarytenoidchanges • Dental erosion • Subglottic stenosis • Laryngealcancer Vaezi MF, Hicks DM, Abelson TI, Richter JE. Clin Gastro Hep 2003;1:333-344.
Odontologia Dental erosion Pchyatric Sleep disorders Sexual disorders Anxiety Pediatric Recurrent pneumonia Sudden infant death Otitis media Other Bad odor in the mouth Dry mouth
Sleep-related GER • Oesophagitis • Barrett oesophagus • Oesphageal adenocarcinoma • Arousals • Poor sleep quality • Excessive daytime slşeepiness • Deteoriation in quality of life • GER- related exstraoesophageal manifestations
UES in proximality • 18-22 cm. • LES in distality • 3 types of contraction primary secondary non-peristaltic
Transient LES relaxations occur without swallowing • Responsible of 63 % -74 % of GER episodes
Increase in gastric acid secretions Delay in gastric emptying Increase in gastric pressure GER
Large pleural-abdominal pressure gradients • Obesity • Oesophageal dysmotility • LES hypotension • Hiatal hernia GER
Mechanisms of GER-related respiratory symptoms • Nocturnal ascit reflux microaspiration exudative mucosal reaction • Ascid reflux esophagus vagus nerve bronchoconstriction
Respiration is not a static process. • Body position changes pressure conditions. • In some respiratory diseases, subatmospheric intrathoracic pressure increases with volume increase as the result of the increase in respiratory resistance GER
GER AND SLEEP • Sleep-related GER in patients with GER 79 % • Sleep Heart Health Study 25 % • BMI • Consumption of carbonated drinks • snoring • Sleepiness • İnsomnia • Benzodiazepines • HT and asthma Fass R. Chest 2005;127:1658-66
Physiology of sleep-related GER • Basal gastric ascite secretion peaks between 20.00 pm - 1.00 am. • Gastric emptying delays. • No saliva production • No swallowing during stable sleep • UES pressure drops from 44 mm Hg to 10 mm Hg. • During REM sleep UES reflex persists.
LES pressure doesn’t change. • No transient LES relaxations during stable sleep • Esophagus ascite clearance significantly delays during sleep and requires arousal for clearance. • Esophageal ascite migrates toward proximal. Harding SM. Sleep Medicine Clinics 2007; 2:1
Sleep Position Gastric ascite is very close to the esophagus due to the posterior position of the oesophagus.
GER events in wakefulness are frequent but short. • Less frequent in sleep but long . because of the increase in esophageal clearance duration • Eating within the two hours before sleep
Sleep is a risk factor for GER. • No difference between REM and NREM • More frequent in the first half of sleep • More frequent in lateral decubitus position Demeter P, Pap A. J Gastroenterol 2004;39:815-20 Hila A. J Clin Gastroenterol 2005; 39:579-83 Demeter P, Pap A. J Gastroenterol 2004;39:815-20
Ascite production increases in wakefulness. • LES pressure decreases as sleep deepens in healthy volunteers. Kahrilas PJ,et.al. Gastroenterology 1987;92:466-71 Stacher G,et al. Gastroenterology ; 1975;68:1449-55
Diaphragma is related with LES through PEL . • Respiratory work of diaphragma increases during OSA • Cardia is affected due to frequent changes in PEL position cardia insufficiency • Deteoriation in swallowing
Obesity and alcohol abuse increase intraabdominal pressure and decrease in oesophageal clearance
Sleep-related GER and OSAS • Obstructive apnea episodes in parallel with the increase in intrathoracic pressure transdiaphragmatik pressure increases effect on phrenooesophageal • Pressure changes cardia insufficiency gastric volume clearance LES insufficiency GER
Serious respiratory symptoms without typical upper GIS complaints • Awakening at sleep with panic choking and ascitic burning
2000 adults, 20-44 age • Snoring in 5 % of males and 2 % of females • Apneas in patients with GER
GER symptoms are more frequent in older patients with OSA than without OSA. Teramoto et al. J Am Geriatr Soc 1999; 116: 17-21
OSAS + GER CPAP decrease in reflux events • OSA, may be a causal factor for GER. Green BT. Arch Intern Med 2003;13:41-5
Reflü Arousal • GER causes OSA • OSA + GER , 20 mg omeprazol 2x1 • Improvement in AHI in 30 % of the cases Kerr P. Chest 1992;101:1539-44
10 cases with OSAS • OSAS + GER in 8 • 20 mg omeprazol 2x1, 2.7 months + diet • Significant improvement in EDS Demeter P, Pap A. J Gastroenterol 2004;39:815-20
CPAP, can decrease GER in cases with OSAS by increasing intraoesophageal pressure. • Seropositivity for Helicobacter pylori has been found to be significantly high in patients with OSAS. Ünal M. Clin Otolaryngol 2003;28:100-2
OSA Dph (-) pTh PEL pTD TLESR (n) GER
Oesophageal and tracheal ascit affects airway reactivity and peak expiratory flow rates during sleep. • In patients with GER + nocturnal asthma, when oesophageal pH drops, PEFR 8 L/m in the monitorization of oesophageal and tracheal pH • When tracheal pH drops , PEFR 84 L/m
Diagnosis of Sleep-Related GER • Careful history • Oesophageal pH test • Endoscopy • PSG
Esophageal pH monitorization • 24 hours • pH < 4 GER • Distal esophagus probe is placed 5 cm above the LES. • Manometric determination of LES is gold standard for the placement of pH probe.
A reference lead is placed on the anterior chest wall and the esophageal pH probe is then connected to a portable data acquisition device that has an event marker that the patient pushes to note when symptoms occur.
Wireless, Catheter-Free Esophageal pH Monitoring Potential Advantages • Improved patient comfort and acceptance • Continued normal work, activities and diet study • Longer reporting periods possible (48 hours) • Maintain constant probe position relative to SCJ
63 pts with OSA ( AHI > 15 ) • 41 controls • 47% of GER events has no relation with apneas • 11 % were preceded within 1 minute of apneic events • 30 % were followed by apneic events • 12 % occurred simultaneously
Treatment • Conservative measures • Medical treatment • Proton pump inhibitors • H2 receptor antagonists, prokinetic agents • Surgical treatment • Fundoplication
Future medications GABA antagonists Baclofen
Open and laparoscopic Nissen fundoplication • Symptom resolution in 80 % to 90 % of GER patients • Complications • Dysphagia • Chest herniation • Vagal nerve damage
62 % of surgically treated patients still require GER medication postoperatively. • Endoscopic fundoplication is considered experimental. Rothstein R. Gastroenterology 2006;131:704-12
Management strategy for sleep-related GER • Conservative measures + PPI (30-60 min before dinner) prokinetic agent esophageal pH testing