Download
1 / 30
340 likes | 654 Views
Skin, Hair& Nails. Presented by: Tagreed marji. Skin:. has 2 layers-outer(epidermis)& inner supportive dermis. Beneath a third the subcutaneous layer of adipose tissue. Epidermis :.

E N D
Skin, Hair& Nails • Presented by: Tagreed marji
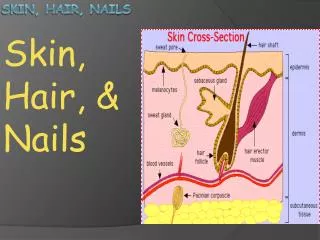
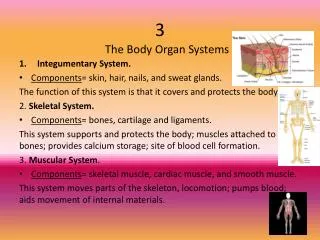
Skin: • has 2 layers-outer(epidermis)& inner supportive dermis. Beneath a third the subcutaneous layer of adipose tissue.
Epidermis: • a protective barrier, contain melanin, thin except on the surfaces exposed to friction, as palms &soles, it’s a vascular, nourished by blood vessels in the dermis below. Skin color is derived from three sources: • brown from melanin.s • yellow from carotene. • red-purple from underlying vascular bed.
Dermis: • it’s the inner supportive layer consist of collagen that allows skin to stretch. • nerves, sensory receptors, blood vessels, lymphatic.
Subcutaneous layer: • adipose tissue(fat cells), for temperature control& cushion effect, also increased mobility
vEpidermal appendages: • - hair- Sebaceous Glands (sebum)- Sweat Glands(eccrine produce sweat & apocrine produce milky secretion into hair follicles when have emotional &sexual stimulation)- Nails.
Nails • Posterior nail fold &lateral • Nail plate & nail matrix • Nail bed • lunula
1- protection from physical, chemical, thermal & light sources. 2-Prevent penetration of microorganisms & loss of water& electrolytes. 3-Perception: sensory surface for touch, pain, temperature… 4-Temperature regulation: through sweat glands& heat storage 5- Identification: facial characteristics, color& fingerprints. 6Communication:non verbal communication (facial expression, body posture) 7- Wound repair: cell replacement 8- Excretion of metabolic waste 9-Production of vitamin D(ultraviolet light convert cholesterol into vitamin D vFunctions of the Skin:
** Subjective Data: • 1. previous hx of skin disease as allergies • 2. change in color or pigmentation, generalized change suggests systemic illness(pallor-jaundice-cyanosis). • 3. change in mole: suggest neoplasm. • 4. Excessive dryness or moisture: seborrhea-oily, xerosis- dry.
5. purities: where &when it start, occurs with dry skin, aging, drug reactions, lice. Scratching may cause excoriation of primary lesion • 6. excessive bruising: where on the body- how did happen—how long you had it, possibility of abuse or dizziness of neurological or cardiovascular origin.
7. rash or lesion: onset- location- where spread- quality- color- tender-warm- duration-anyone at home or work with similar rash, tried new food? identify primary site. 8. medications: prescription & over-the- counter, how long on medication.drugs may increase sun light sensitivity as thiazides diuretics
9. hair loss: a gradual or sudden onset? symmetrical? unusual hair growth? Alopecia -Hirstuisim 10. change in nails: shape-color brittleness 11. Environmental or occupational hazards: as dyes, chemicals, radiation, sun exposure, insect bitten, exposure to plants, animals? may result a skin neoplasm people at risk: farmers-sailors- those over 40.
12. self-care behaviors: cosmetics-soap-chemicals usage. • Danger signs: ABCDE • Asymmetry of lesion • Border • Color variation • Diameter • elevation
** Objective data: • Preparation: equipment needed; direct lighting(natural daylight is ideal but not always available)- ruler-penlight-gloves. • Comprehensive physical exam: skin assessment is integrated throughout the complete exam, at the beginning assessing hands &fingernails, to accustom him to your touch. Inspect toes &its nails too. • The regional exam: remove his clothes, stands back at first to get an overall impression, to reveal distribution pattern. inspect mucous membrane too.
· External variables influencing skin color(projector) • -Emotions as fear cause vasoconstriction → false pallor • -Environment as hot room cause vasodilatation → false Erythema • -Physical as prolonged elevation cause decreased arterial perfusion → pallor whereas dependent position cause venous pooling→ redness.
** INSPECT & PALPATE SKIN: • Color: normally consistent with genetic background, examples; • a.Freckles__ small ,flat macules of brown melanin pigment that occur on sun exposed skin. • b.Mole__ a proliferation of melanocytes , tan to brown color, flat or raised • c.Birthmarks__ tan to brown in color.
# Color change: note if it transient or is due to pathology. • a.Pallor: when red-pink tones from the oxygenated hgb in the blood are lost, skin takes collagen color(white),causes: stress-smoking • generalized pallor can be observed in the mucous membranes, lips , conjunctiva& nailbeds.
B. Jaundice: • a yellow color indicating rising amounts of bilirubin in the blood, first noted in the hard & soft palate in the mouth & sclera.
C. Cyanosis: • a bluish color, the tissues are not adequately perfused with oxygenated blood.
D.Erythema: • intense redness due to excess blood(hyperemia) in the detailed superficial capillaries, expected with fever , local inflammation or emotional reactions.
Skin assessment:cont • # Temperature: use the backs(dorsa) of your hands bilaterally, should be warm . • -hypothermia ≡ hyperthermia • # Moisture: moist appears normally on the face, hands, axilla& skinfolds in response to activity, a warm environment or anxiety. Diaphoresis as in heavy activity or fever. Dehydration in oral mucous membranes. • # Texture:smooth & firm with an even surface.
# Thickness: epidermis is uniformly thin. A callus is a circumscribed overgrowth of epidermis & is an adaptation to excessive pressure from the friction of work . • # Edema: fluid accumulating in the intercellular spaces, imprint your thumbs firmly against the ankle malleous or tibia. normally the skin surface stays smooth. If your pressure leaves a dent in the skin, pitting edema is present, graded on 4 points scale:
Edema: • + 1: mild pitting • +2 moderate • +3 deep • +4 very deep
# Mobility & Turgor: pinch up a large fold of skin on the anterior chest under the clavicle, mobility is the skin’s ease of rising & turgor is its ability to return to place promptly when released, this reflects the elasticity of skin. • # Vacularity or Bruising: angiomas , smooth, slightly raised bright red dots that commonly appear on the trunk in all adults over 30.
# Lesions: • note the; color-elevation-shape- size- location& distribution-any exudates.
** INSPECT & PALPATE THE HAIR: • -color • - texture • - distribution • -lesions
** INSPECT & PALPATE THE NAILS: shape & contour: normally slightly curved or flat, edge are smooth, rounded& clean
Nails assessment: • a.the profile sign: index finger note the angle of the nail base, it should be about 160 degrees, curved nails with a convex profile • B. consistency: surface is smooth & regular, not brittle or splitting, firmly adhere to the nail bed.
C. Color:even, pink nail bed underneath. All people normally may have white hairline linear markings from trauma or picking at the cuticle. d. Capillary refill: depress nail edge to blanch then release noting return of color, return is instant, or at least within a few seconds in a cold environment, indicates the status of the peripheral circulation.
*** skin lesions: • ** Primary &secondary lesions • page 176-185