Download
1 / 111
1.11k likes | 1.31k Views
LYME DISEASE and Tick-born Co-Infections Dr. Emily Maiella 413.230.4462. Introduction. What is Lyme Disease How is "Lyme Disease" Contracted How prevalent is "Lyme Disease" What are the co-infections and co-morbid conditions What are the symptoms of "Lyme Disease"

E N D
LYME DISEASE and Tick-born Co-Infections Dr. Emily Maiella 413.230.4462
Introduction • What is Lyme Disease • How is "Lyme Disease" Contracted • How prevalent is "Lyme Disease" • What are the co-infections and co-morbid conditions • What are the symptoms of "Lyme Disease" • How is "Lyme Disease" diagnosed • How is "Lyme Disease" treated • Allopathically • Naturopathically • Can you/should you treat Lyme Disease? • Who are Lyme friendly/Lyme Literate Physicians
Introduction Continued • I want you to walk away from this presentation with • a better understanding of what "Lyme Disease" is • a realization that it is becoming more common everywhere • realize how important it is to treat it effectively when it is acute, and that chronic Lyme Disease needs to be managed by a "Lyme Literate" specialist physician. • That currently this issue is highly political and needs advocates!
Lyme DiseaseTHE POLITICS There are currently 2 schools of thought on Lyme Disease and the issue is highly political. IDSA, "The International Disease Society of America" despite growing evidence to the contrary continues to conclude that: 1. lyme disease is over diagnosed 2. that it is over treated 3. that chronic lyme does not exist 4. that there is no evidence for repeated treatments or prolonged treatments.
Lyme DiseaseTHE POLITICS The second camp: ILADS, "The International Lyme and Associated Diseases Society" based on continually updated clinical and laboratory evidence, recognizes that • chronic lyme disease does exist • that there is evidence for repeated treatment when relapse occurs • and that there is evidence for prolonged treatment.
THE POLITICS All patients with LD must be alerted to the 2 schools of accepted treatment and allow them to decide which they want to follow I see validity in both schools. While I do advocate for prolonged antibiotics in some cases, I do not think that antibiotics alone, can cure advanced Lyme disease. Even with acute cases, I never use antibiotics without herbs.
Lyme Disease Defined • Traditionally, Lyme disease is defined as an infectious illness caused by the spirochete, Borrelia burgdorferi • This is technically correct; clinically the illness is much more than that, especially in the disseminated and chronic forms. • This includes infection not only from B. burgdorferi, but the many co-infections that may also result. • Furthermore, in the chronic form of Lyme, other factors can take on an ever more significant role; immune dysfunction, opportunistic infections, co-infections, biological toxins, metabolic and hormonal imbalances. J. Burrascano; Advanced Topics In Lyme Disease; 15th edition; Sept 2005
Lyme Diseasecomplexity and history • Has been recognized in Europe, especially in Germany, symptomatically & clinically at least back into 18th century. • Borrelia is a spirochete like syphilis • Syphilis was called the "Great Imitator" prior to the advent of antibiotics, due to its ability to affect any body system and therefore mimic many other pathologies • LD has the same capability to affect all body systems and mimic any number of pathologies • Before antibiotics, Physicians who could treat (palliate) syphilis were said to "know medicine". This reference had to do with the fact that so many systems were affected and the knowledge and understanding needed to treat it. • This is also the same with "Lyme Disease", and the complexities of this disease are sufficient to require specialization in this area to treat effectively.
Lyme Borreliosis (LB) • There are over 5 subspecies of Borrelia burgdorferi senso lato, over 100 strains in the US, and 300 strains worldwide. This diversity is thought to contribute to Borrelia's antigenic variability and its various antibiotic resistances. • http://www.pasteur.fr/recherche/borrelia/Borreliaspecies.html (good site for listing strains and locations that various strains are common) • Transmitted by various tick species, mostly deer ticks • Post exposure rashes are found in only 40-60% of cases, and as few as 10% of these rashes are classic erythema migrans ("bull's-eye"). • Infection may cause persistent, recurrent musculoskeletal, neurological, psychiatric and other system symptoms. Johnson & Stricker, Expert Review of Anti-Infect Ther 2004; 2:533-57
www.CDC.gov lyme rash photos single erythema migrans lacking central clearing single erythema migrans with central clearing multiple erythema migrans Erythema Migrans; Pathognomonic for Borreliosis; 'rash' only occurs in 40-60% of people who are bitten and contract Borrelia spp.
Spirochetes characteristics compared Borrelia spp., Treponema pallidum • Borrelia b. has over 1500 gene sequences • At least 133 of these genes are 'functioning genes' • In contrast, T.pallidum (Syphillus) has 22 functioning genes. • Borrelia b. has 21 plasmids; That's 300% (or 3x) more plasmids than any known bacteria!! Casjens S et al., Mol Microbiol 2000, 35:490-516, Porcella & Schwan, J Clin Invest 2001; 107:651-6, Embers et al, Microbes Infect 2004; 6:312-318
How Borrelia evades testing • Stealth Pathology of Borrelia b. includes: • Immune suppression • Phase & antigenic variation • Physical seclusion • Intracellular sites • Extracellular sites • Secreted Factors
Borrelia B. morphological forms and niches • Bb can be found in various niches of the body • fluid compartments (including the eye) • tissue compartments (including CNS, ligaments and tendons) • intracellular • especially within the acidic vacuoles of cells, which Bb forms, where many antibiotics are non-effective • Bb thrives in slightly acidic environments and low oxygen concentration; it is anaerobic. • Bb is also heat labile and is inactivated/destroyed at temperatures of 104 F for 3 hours • Bb currently has a number of recognized life forms • Spirochete form • L-form aka spheroplast (cell wall deficient) • cyst form (also cell wall deficient), which allows dormancy until favorable conditions arise. Donta St, Tetracycline therapy for chronic lyme disease, Clinical Infectious Disease 25: suppl 1(July 1997):352-356
Borrelia burgdorferi the spirochete that causes Lyme Disease. FA stain and darkfield microscopy (CDC) Spirochetes: B.burgdorferi and T.Pallidum A scanning electron micrograph of T. pallidum
Functional Characteristics of Bb • Often an intracellular organism • Avoids antibody detection and avoids lysis from most beta lactam abx which do not penetrate cells. Bb is not present in high numbers in the blood. (Penicillins・Cephalosporins・Cephamycins・Carbapenems・Monobactams・Beta-lactamase inhibitors) • Dorward D, 9th International Conference on Lyme Borreliosis, 1998 • Microaerophilic • Helical Bb will tend to move away from oxygen-rich areas in vivo and reside in fascia, cartilage, epineureum and other oxygen poor areas. • Barbour AG et al "Borrelias Strategies for Survival", Science 1987, No 237, pp 403-411 • Heat Sensitivity • Helical Bb may be inactivated and destroyed upon exposure to temperatures of 104 F for 3 hours • Hyperthermia was also used successfully in the treatment of syphilis prior to antibiotics • Barbour AG, et al. Science 1987 • From Mercury to Malaria to Penicillin: The History of the Treatment of Syphilis at the Mayo Clinic, 1916-1955
Functional Characteristics of Bb Cont. • Epitope switching: Bb alternates its outer surface proteins preventing sustained immune recognition and attack. • Seller et al, "Immunity to Lyme Disease: Protection, pathology and persistence. Current opinion in Immunology 1996, 8(4): 503-9 • Stress mediated toxin release: Jarisch-Herxheimer reactions can complicate treatment, as well as clinically guide physicians in diagnosis and effectiveness of treatment.
Functional Characteristics of Bb Cont. • Slow Division Cycle: In vitro (in test tube) generation time is 12-36 hours, in vivo (in life) is much longer; perhaps 14-28 days. • Chiao JW, Abstract 7th International Conference on Lyme Borreliosis, 1994: Defosse DL et al. "In vitro and in vivo induction of TNF alpha by Bb" Infect Immun 1992; 60: 1109-1113 • Bb surrounds itself with hosts own lymphocyte cell membrane: Avoids detection from host immune system • Doward D. et al. Clinical Infect Dis, 1997 • Bb actively attacks lymphocytes, macrophages, natural killer cells: Destroys bodies defensive weapons • Doward D et al. Clinical Infect Dis, 1997
Where Bb hangs out • Bb is often an intracellular organism • Brouqui P. et al, "Eukaryotic cells protect Borrelia from the action of penicillin and deftriaxone but not from the action of doxycycline and erythromycin" Antimicrob Agents Chemother 1996; 40: 1552-1554 • Bb can thrive within fibroblasts (cells responsible for making connective tissue) • Klempner et al "Invasion of human skin fibroblasts by the Lyme disease spirochete, Borrelia burgdorferi", J Infect Dis 1993; 167: 1074-81 • Bb can thrive within lymphocytes and macrophages (immune cells) • Dorward et al, "Invasion and Cytopathic Killing of human lymphocytes by spirochetes causing lyme disease", Clin Infect Dis 1997; 25 (Suppl 1): S2-8 • Bb can harbor within endothelial cells • Ma et al, "Intracellular localization of Borrelia burgdorferi within human endothelial cells", Infect Immun; 1991; 59: 671-8 • Bb has a proclivity to remain within synovial cells (joints) • Girschick et al, Intracellular persistence of Borrelia burgdorferi in human synovial cells", Rheumatol Int 1996; 16 125-32 • Bb can cross the placenta, can cause congenital infection. • Bb is in breast milk and can cause infection through ingestion.
Functional Characteristics of Bb • Bb selectively binds Oligodendria cells: These cells are responsible for synthesis and maintenance of myelin: In addition to direct destruction of myelin by bacterium, the host antibodies may attack myelin while targeting Borrelia to which myelin is in close contact thus stimulating genuine Multiple Sclerosis • Garcia Monco JC, etal "Adherence of the Lyme Disease spirochete to glial cells and cells of glial origin" J Infect Dis 1989, 160:497-506 • Bb can change its morphology to cell wall deficient cysts which are heat, pressure and oxygen resistant. Cysts are resistant to all abx except Tinidazole, metronidazole (Flagyl) and Hydroxychloroquine (plaquonil.) In vitro Cystic Bb can readily revert back to helical Bb. • Cystic forms of Bb are probably a main reason for treatment resistance and relapse. • Brorson et al. "Transformation of Cystic Forms of Bb to Normal Mobile Spirochetes" Infection 1997, No. 25 pp 240-246
Biofilms • Spirochetes draw upon calcium, magnesium, iron, heavy metals, fibrin and other elements to weave a protective coat around themselves. • They create a “filmy” structure around themselves and shed their outer membrane proteins (which serve as antigens), and are able to evade the immune system and antibiotics
Biofilms • In a biofilm, pathogens are 100-1000 times more antibiotic resistant.
The Alzheimer’s and Autism Connection • Possible link with Alzheimer's Disease: ongoing research, not published yet presented at the AANP 2005 annual convention demonstrated that in 10 post-mortem Alzheimer's patients, 7 of specimens had fusion of DNA from the flagellin of Bb with the human DNA of chromosome 11 producing a Transfection product. Samples were taken from the neurofibrillary tangles within the hippocampus and analyzed with PCR and DNA sequencing. • In 1913 Noguchi and Moore reported Treponema pallidum spirochetes were found in 12 of 70 brains from patient with general paresis.
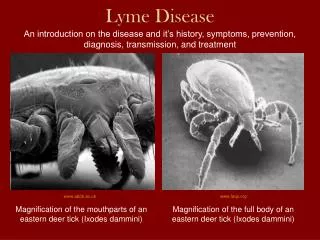
Modes of Transmission • Various species of ticks carry Bb and other pathogens • Ticks known to carry Bb include Ixodes tick spp, Ammblyoma americanum (Western Black Legged tick) and Dermacentor variabilis (Wood/Dog ticks) • Previous studies have demonstrated that a minimum number of hours of attachment needs to take place for transmission to happen based on the time it takes a tick to empty any gut contents into the host. CDC states 24 hrs. • However there is growing clinical evidence that this may not be the case. Clinically/Anecdotally it may take 4 hours or less to contract pathogens from a tick bite. • Pathogens have been located in the salivary apparti of the tick in addition to the GI and may be expelled on initial bite when anodyne and anticoagulant materials are released from the mouth.
Speculated Modes of Transmission • Dietrich Klinghardt M.D., Ph.D., refers to a study in Czechoslovakia in which 15% of mosquitoes tested carried Borrelia spp. (I have not been able to find the study, however it may be in Czech). • There is speculation based on patient exposure and clinical information, although unstudied, of other insects being vectors. • Clinically many "Lyme Literate" physicians observe that Lyme Disease happens in family clusters. What is not known is whether there are common exposures, or other routes of transmission that are yet unidentified/unstudied. • Another thought is that perhaps the infection is highly prevalent and that certain genotypes predispose to infection developing into disease (HLA typing correlation, genetic detox pathway dysfxn).
Only 15%-50% of people with diagnosed "lyme disease" recall having been bitten by a tick. Recall that a rash occurs only in 40-60% of those with LD. It is very easy to miss having been bitten by a tick due to the small size in the nymph and larval stages of their lives. Bitten by the Vector
The Vector • Ixodes scapularis (Deer Tick) • Deer ticks have a two-year life cycle. That is, it takes two years for one egg-adult-egg generation to evolve. Therefore, deer ticks can be found all year long, including wintertime. www.canlyme.com
Prevalence ofticks and Lyme Disease Lyme disease is prevalent across the United States. Ticks do not know geographic boundaries. A patient's county of residence does not accurately reflect their total Lyme disease risk, since people travel, pets travel, and ticks travel. This creates a dynamic situation with many opportunities for exposure for each individual. Over 40 species of migratory birds have been found to carry the various spp. of ticks that carry lyme disease pathogens ILADS website
Prevalence of LD & Ixodes ticks nationwide through 2002 based on CDC surveillance Distribution of Ixodes ticks that transmit Lyme disease in the U.S. (CDC)
How Under Reporting occurs
Inclusion criteria for reporting for surveillance: erythema migrans OR late stage symptoms PLUS Isolation of Bb from clinical specimen ie. PCR (high specificity but 20% or less sensitivity unless done on EM lesion) OR +ELISA (40-70% sensitivity) PLUS+Western Blot (40-70% sensitivity) Alaska 19 Arizona 44 California 3,053 Colorado 12 Connecticut 39,325 Idaho 93 Minnesota 6,688 New York 78,791 New Mexico 30 Oregon 278 Utah 41 Washington 235 Prevalence of "LD" reported to the CDC from 1980-2005;
http://www.cdc.gov/ncidod/dvbid/lyme/ld_rptdLymeCasesbyState.htmhttp://www.cdc.gov/ncidod/dvbid/lyme/ld_rptdLymeCasesbyState.htm Check it out for your state!
Prevalence & Cost of Lyme Disease in U.S. and Worldwide • CDC estimates that their disease reporting inclusion criteria in actuality only represents 1/10 to 1/100 of the actual cases that are either undiagnosed or are clinically diagnosed and don't fit the surveillance criteria and as such go unreported. • The CDC surveillance criteria were devised to track a narrow band of cases for epidemiologic change and were never set up to be used as diagnostic criteria nor were they meant to define the entire scope of Lyme disease. This is stated in the 3/25/91 NIH report. Klaus-Peter Hunfeld, M.D., PhD 2005 ILADS presentation
Tick Born Co-infections A typical co-infection panel that I suggest includes: • B. microti and B. duncani (WA-1): for Babesia • B. henselae and B. Quintana IgM and IgG: for Bartonella • Anaplasma phagocytophila IgM and IgG: for human granulocytic Ehrlichiosis (HGE) • Ehrlichia chaffeensis Ab IgM and IgG: for Human monocytic Ehrlichiosis (HME) • The presence of co-infection points to probable Lyme infection, and when left untreated, increases morbidity and complicates successful treatment of Lyme Disease. Lyme panels can include co-infection testing through Igenex, Immunosciences and MDL.
Co-Infections with Lyme Disease • Although not true co-infections, viral infections are often re-activated when Lyme is active, so testing and treating for herpes family viruses, EBV, CMV, as well as candida is important. • CO-INFECTIONS HAVE SIMILAR SYMPTOM PRESENTATIONS TO LD, HOWEVER SOME SYMPTOMS MAY BE MORE PRONOUNCED. CONSIDER CO-INFECTIONS IF THE FOLLOWING SYMPTOMS ARE PRONOUNCED, OR TREATMENT FOR Bb ALONE IS NOT EFFECTIVE.
Babesia • Babesia: intra-cellular Malaria like protozoal organism. Infects red cells. It is thought that 2/3 of Lyme pts have Babesia, which is hard to diagnose as there are over 17 antigen different subspecies and the only current tests cover only B. microti and WA-1, which are the most common in western US states. • Sx's: vertigo, headache, fatigue, dental problems, TMJ problems, eye problems (floaters & blurry vision), weight loss, abdominal problems, fibromyalgia, SOB, frequent coughing/sighing, malaise, drenching night sweats, violent nightmares, vivid dreams, recurrent high fever and chills • Diagnosis: via FISH test or WA-1 test through Igenex, MDL or Immunosciences. Some people use long term observation of blood under darkfield microscope as Babesia leaves dying cells which can be observed under darkfield. • Treatment: Rx's: Mepron and other antimalarial drugs and Artemisinin (200-300 mg bid 3 wk on/1 wk off taken with grapefruit juice) is used and has been shown in studies to be 20% more effective for malaria than the pharmaceutical treatments. Use with boneset (best way is a hot tea)
Cryptolepsis • From Ghana • Used in Africa for thousands of years to treat (and prevention) for malaria. • Safe for children. • Has a spiral in flowers. • 30-40 drops tid, but start lower. • Colors cloth in africa
Bartonella • Bartonella: causative organism is B. henselae and B. quintana. Also known as "Cat Scratch Disease" as it transmits between humans and cats. • Pronounced Symptoms Include: plantar fascial pain, swollen glands, endocarditis, anxiety/psychiatric symptoms, neuropathy/Reflex Sympathetic Dystrophy, ice-pick-like headaches, major photophobia, hepatitis, neovascularization, fatigue, low grade fever, jaw bone cavitations, devitalized teeth, often a co-infection in ALS, fibromyalgia and joint pain. Summing up: anxiety (over-riding symptom), with burning neuropathic pain….think Bartonella. • Diagnosis: Antibody or Antigen testing for the organism, best done again through Igenex, MDL, or Immunosciences. • Treatment: Rx's: Zithro, Doxy and Rifampin together; herbal support includes, Polygonum and Stephania root along with supportive treatment.
Ehrlichiosis • Ehrlichiosis: human granulocytic Ehrlichiosis (HGE) is caused by Anaplasma phagocytophila. Human monocytic Ehrlichiosis (HME) is caused by Ehrlichia chaffeensis. Often found in Lyme patients who have contact with horses and farm animals. • symptoms include: fever after initial infection, myalgia and arthralgia, headache, leukopenia and thrombocytopenia, hyponatremia, mental confusion, skin rashes – including genital and oral ulcers, severe pain syndromes, nausea and vomiting (acute flare ups). • Diagnosis: Antibody or Antigen testing for the organism, best done again through Igenex, MDL, or Immunosciences. • Treatment: Various Pharmaceutical antimicrobials; astragalus and colchicine
What some people are diagnosed with instead Lyme disease is the latest great imitator and should be considered in the differential diagnosis/etiology of: • MS • 89% of Dietrich Klinghardt MD PhD patients with previous MS Dx test + for lyme disease • T. Grier PhD in MN is conducting a study not yet published which so far has shown an 80% correlation between MS and Lyme. • ALS • Parkinsons Disease • other neurologic conditions • chronic fatigue syndrome • fibromyalgia • hypochondriasis • somatization disorder • patients with difficult-to-diagnose multi-system syndromes • difficult to treat viral/fungus infections (EBV, HHV's, CMV, candida, mycoplasma spp. etc.)
Stages of Lyme Disease • Early localized: single EM or rash with no constitutional symptoms. Treat promptly and aggressively referring to ILADS or IDSA guidelines. • Early Disseminated disease: multiple lesions, constitutional symptoms, lymphadenopathy, or any other manifestations of dissemination that are 'mild' and present for less than one year, are not complicated by immune deficiency or prior steroid treatment. Refer to a "Lyme Literate Physician.” • Late Disseminated disease: Symptoms present for more than one year, more severely ill patients, and those with prior significant steroid therapy or impaired immunity secondary to lyme disease or any other reason. REFER to lyme literate physician and co-manage with their direction.
Symptoms in Lyme Disease • Every organ & organ system can be affected This is a list of some of the LD symptoms by body system and is not an exhaustive compilation of possible symptoms • Neuro: headaches, facial paralysis, seizures, meningitis, stiff neck, burning, tingling or prickly sensations (parathesia), loss of reflexes, or possible increased or normal reflexes with slow return, loss of coordination and equilibrium. • Neuropsych: mood swings, irritability, anxiety, rage ("Lyme Rage"), poor concentration, cognitive loss, memory loss, loss of appetite, mental deterioration, depression, disorientation, insomnia and numerous mood and psychiatric disorders that were not present prior to lyme disease or are extremely exacerbated by lyme disease. • Head: Headache, neck pain, facial pain and paralysis, difficulty chewing, pain in teeth, dry mouth, decreased sense of taste and smell, numb tongue/mouth, peculiar metallic, salty and other tastes in mouth are also common • Eyes: Pain due to inflammation (scleritis, uveitis, optic neuritis), dry eyes, sensitivity to light, ptosis of eyelids, conjunctivitis, blurry or double vision, floaters, difficulty with eye teaming and convergence, swelling around eyes/bags below eyes.
Symptoms in Lyme Disease • Ears: pain, hearing loss, tinnitus, noise sensitivity, dizziness and equilibrium disorders. • Throat: chronic sore throat, swollen glands, cough, hoarseness, difficulty swallowing • Cardio: weakness, dizziness, irregular heart beats, myocarditis, pericarditis, palpitations, heart block, enlarged heart, fainting, shortness of breath, chest pain, mitral valve prolapse, vasculitis • Respiratory: pleurisy, chest pains, respiratory infections, cough, asthma, pneumonia • Abdomen: pain, diarrhea, nausea, vomiting abdominal cramps, anorexia, liver infection/hepatitis, elevated liver enzymes, enlarged spleen • Urinary: pain with urination, prostate pain, recurrent UTI's, interstitial cystitis • Reproductive: swollen testicles, irregular or ceased menses, galactorrhea, • Musculoskeletal: arthralgias, fibromyalgia • Derm: EM, single or multiple rash, erythema migrans chronicum, hives, ACA • Pregnancy: infertility, miscarriage, premature birth, birth defects, stillbirth • Constitutional: marked fatigue, nights sweats, recurrent fevers
Diagnosis • ILADS Guidelines: based on clinical diagnosis via a scoring method. Points are added up based on exposure/possible exposure, EM, symptoms consistent with lyme, and labs are tallied. 7 or above is highly likely Lyme. 5-6 is possible, and 4 and below is unlikely. • But remember, if you do see a bulls-eye rash, you do not need any testing.
Diagnosis • IDSA Guidelines: Still concludes that it is a clinical diagnosis, but rarely will treat someone with a positive Lyme titer. Figure that one out! • Patients who are diagnosed by IDSA guidelines are treated typically with 100 mg Doxycycline bid for 2-3 weeks and if they have symptoms after treatment are frequently told that it is "post lyme syndrome" (and not Lyme Disease) even though the researchers who helped develop IDSA guidelines have in their own studies shown positive culture in post treatment symptomatic individuals.
Laboratory Tests • The ELISA test is unreliable, and misses 35% of culture proven Lyme (only 65% sensitivity!) and is unacceptable as the first step of a two step screening protocol. (By definition a screening test should have 95% sensitivity.) • Of patients with acute culture proven Lyme disease, 20-30% remain seronegative on serial Western Blot sampling. Antibody titers also appear to decline over time; thus, the IgG Western Blot is even less sensitive in detecting chronic Lyme infection yet the IgM Western Blot may work. For "epidemiological purposes" the CDC eliminated from the Western Blot analysis the reading of bands 31 and 34. These bands are so specific to Borrelia burgdorferi that they have been chosen for vaccine development. However, for patients not vaccinated for Lyme, a positive 31 or 34 band is highly indicative of Borrelia burgdorferi exposure. • When used as a part of a diagnostic evaluation for Lyme disease, the Western Blot should be performed by a laboratory that reads and reports on all 16 bands as part of their routine comprehensive analysis. • "Two Year Eval of Bb Culture and Supplemenary Tests for Definitive Diagnosis of Lyme Disease", Coulter et al; • Journal of Clinical Microbiology; Oct 2005, 5080-5084 • ILADS annual conference and guidelines