Download
1 / 1
10 likes | 179 Views
A Population-based Analysis of Dalteparin Pharmacokinetics in Pediatric Patients at Risk for Thromboembolic Events. J.S. Barrett, L.G. Mitchell, D. Patel, P. Cox, P. Vegh, M. Castillo, P. Massicotte

E N D
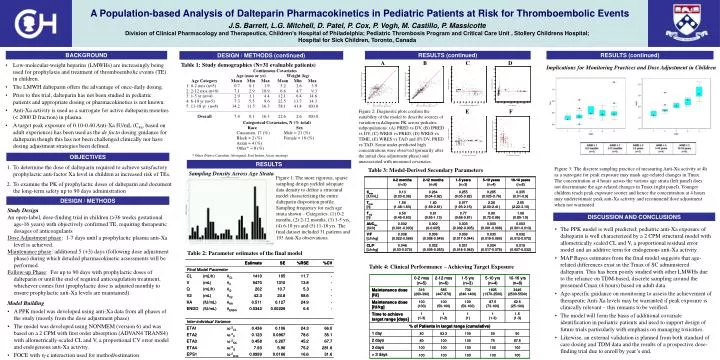
A Population-based Analysis of Dalteparin Pharmacokinetics in Pediatric Patients at Risk for Thromboembolic Events J.S. Barrett, L.G. Mitchell, D. Patel, P. Cox, P. Vegh, M. Castillo, P. Massicotte Division of Clinical Pharmacology and Therapeutics, Children’s Hospital of Philadelphia; Pediatric Thrombosis Program and Critical Care Unit , Stollery Childrens Hospital; Hospital for Sick Children, Toronto, Canada RESULTS (continued) BACKGROUND RESULTS (continued) DESIGN / METHODS (continued) • Low-molecular-weight heparins (LMWHs) are increasingly being used for prophylaxis and treatment of thromboembolic events (TE) in children. • The LMWH dalteparin offers the advantage of once-daily dosing. • Prior to this trial, dalteparin has not been studied in pediatric patients and appropriate dosing or pharmacokinetics is not known. • Anti-Xa activity is used as a surrogate for active dalteparin moieties (< 2000 D fraction) in plasma. • A target peak exposure of 0.10-0.40 Anti-Xa IU/mL (C4h, based on adult experience) has been used as the de facto dosing guidance for dalteparin though this has not been challenged clinically nor have dosing adjustment strategies been defined. A B C D Table 1: Study demographics (N=31 evaluable patients) Implications for Monitoring Practices and Dose Adjustment in Children E F Figure 2: Diagnostic plots confirm the suitability of the model to describe sources of variation in dalteparin PK across pediatric subpopulations: (A) PRED vs DV, (B) IPRED vs DV, (C) WRES vs PRED, (D) WRES vs TIME, (E) WRES vs TAD and (F) DV, PRED vs TAD. Some under-predicted high concentrations were observed (primarily after the initial dose adjustment phase) and unassociated with measured covariates. * Other (Native Canadian, Aboriginal, East Indian, Asian, missing) RESULTS • To determine the dose of dalteparin required to achieve satisfactory prophylactic anti-factor Xa level in children at increased risk of TEs. • To examine the PK of prophylactic doses of dalteparin and document the long-term safety up to 90 days administration Figure 3: The discrete sampling practice of measuring Anti-Xa activity at 4h as a surrogate for peak exposure may mask age-related changes in Tmax. The concentration at 4 hours across the various age strata (left panel) does not discriminate the age-related changes in Tmax (right panel). Younger children reach peak exposure sooner and hence the concentration at 4 hours may underestimate peak anti-Xa activity and recommend dose adjustment when not warranted. Table 3: Model-Derived Secondary Parameters Sampling Density Across Age Strata Figure 1: The more rigorous, sparse sampling design yielded adequate data density to define a structural model characterizing the entire dalteparin disposition profile. Sampling frequency for each age strata shown – Categories: (1) 0-2 months, (2) 2-12 months, (3) 1-5 yrs, (4) 6-10 yrs and (5) 11-18 yrs. The final dataset included 31 patients and 193 Anti-Xa observations. • Study Design • An open-label, dose-finding trial in children (>36 weeks gestational age-16 years) with objectively confirmed TE, requiring therapeutic dosages of anticoagulants • Dose Adjustment phase: 1-7 days until a prophylactic plasma anti-Xa level is achieved. • Maintenance phase: additional 5 (+3) days (following dose adjustment phase) during which detailed pharmacokinetic assessments will be performed. • Follow-up Phase: For up to 90 days with prophylactic doses of dalteparin or until the end of required anticoagulation treatment, whichever comes first (prophylacticdose is adjusted monthly to ensure prophylactic anti-Xa levels are maintained). • Model Building • A PPK model was developed using anti-Xa data from all phases of the study (mostly from the dose adjustment phase) • The model was developed using NONMEM (version 6) and was based on a 2 CPM with first order absorption (ADVAN4 TRANS4) with allometrically-scaled CL and V, a proportional CV error model and endogenous anti-Xa activity. • FOCE with - interaction used for method/estimation Table 2: Parameter estimates of the final model Table 4: Clinical Performance – Achieving Target Exposure






















