Download
1 / 9
110 likes | 271 Views
Celiac Disease. Ben Greenfield 28 September 2013. Epidemiology. 1% of the population in North America More common in the Caucasian population, very rare in Asian and African populations More common in females Most often presents from 9-18 months, but may present any time. Pathophysiology.

E N D
Celiac Disease Ben Greenfield 28 September 2013
Epidemiology • 1% of the population in North America • More common in the Caucasian population, very rare in Asian and African populations • More common in females • Most often presents from 9-18 months, but may present any time
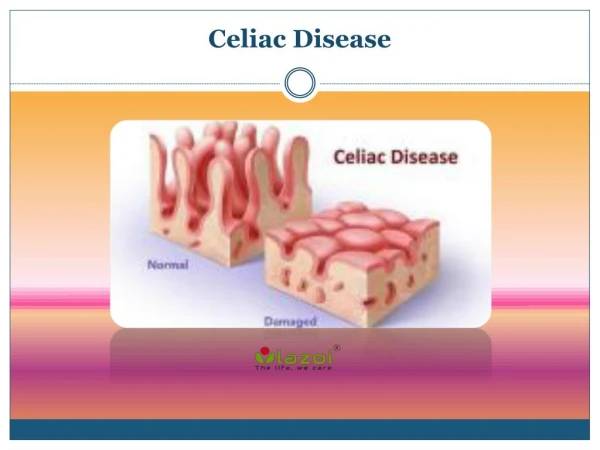
Pathophysiology • Autoimmune response against tissue transglutaminase (tTG) • Gluten triggers the autoimmune response • Associated with HLA DQ-2 gene (or DQ-8 sometimes) • Small intestine is most affected • Mucosal layer is affected • Lymphocystosis within epithelial cells, hyperplasia of crypts, and atrophy/blunting of villi is observed
Presentation • Commonly presents with diarrhea, vomiting, abdominal pain +/- abdominal distention • Can present with more severe symptoms secondary to malnutrition such as weakness due to muscle wasting or lethargy. • Can be “silent” without any manifestations.
Diagnosis/Findings Diagnosis • First: anti-tTG, anti-endomysial antibodies (EMA) – if anti-tTG is 10x greater than normal and + EMA, biopsy may not be required for diagnosis • Endoscopic biopsy (at least 4 samples) – see staging on next slide Other Possible Findings • Low potassium, calcium, folate, magnesium, vitamin D, vitamin K, albumin, zinc • Normal B12
Staging Type 0 = Pre-infiltrative stage (normal tissue) • Type 1 = Infiltrative lesion (increased lymphocytes within epithelial cells) • Type 2 = Hyperplastic lesion (same as type 1, but also with hyperplastic crypts) • Type 3 = destructive lesion (same as type 2, but also with atrophy of villi) – there are sub-categories of a, b, and c, based on increasing severity of atrophy.
Management • Lifelong avoidance of gluten containing foods (wheat, rye, barley) • Temporary vitamin supplementation may be required • Lactose avoidance until symptoms are well-controlled by gluten-free diet • Monitoring for other autoimmune diseases- refer to endocrinologist as needed • Steroids for severe or refractory symptoms • Topical dapsone for dermatitis herpetiformis
Complications • Lactose intolerance • Malignancy – Small bowel lymphoma is highest risk; also, esophageal cancer, small bowel adenocarcinoma • Anemia • Miscarriage • Osteomalacia, osteopenia, osteoporosis
References • S Guandalini, C Cuffari, S Schwarz, P Vallee, J Vargas. “Pediatric Celiac Disease.” Medscape. 18 April 2013. Web. 28 September 2013. • Murphy S, Walker A. “Celiac Disease” Pediatrics in Review 1991;12;325-330. Web. 24 September 2013