Download
1 / 30
380 likes | 739 Views
Lindsey Albenberg, DO Ritu Verma, MD The Children’s Hospital of Philadelphia Reviewed by Edward Hoffenberg, MD of the Professional Education Committee. Celiac Disease. Case. 14 month old F with FTT Watery diarrhea x 2 months; 3-10 episodes per day; stool infectious work-up by PCP negative

E N D
Lindsey Albenberg, DO Ritu Verma, MD The Children’s Hospital of Philadelphia Reviewed by Edward Hoffenberg, MD of the Professional Education Committee Celiac Disease
Case • 14 month old F with FTT • Watery diarrhea x 2 months; 3-10 episodes per day; stool infectious work-up by PCP negative • No nausea, vomiting, abdominal pain, abdominal distention, hematochezia, melena • No improvement in symptoms with change to soy milk • No significant PMH or FH • PE: Pale skin, abdomen distended but soft and nontender, normal bowel sounds, no organomegaly Celiac Disease
Growth Chart Celiac Disease
Labs • WBC 14.1, Hgb9.7, Plt 392; normal MCV and iron studies • AST 30, ALT 23, T bili 0.2, albumin 2.8 • Hemoccult negative, stool WBC negative, spot fecal fat test positive • Celiac Panel • IgA 69 (14-105) • Endomysial AB Positive • Tissue TransglutaminaseIgA AB 190.5* * Negative = < 20 Indeterminate = 20-40 Positive = > 40 Celiac Disease
What is Celiac Disease? • Auto-immune condition • Occurs in genetically susceptible individuals • A unique autoimmune disorder because… • Environmental trigger (gluten) and the autoantigen (tissue-transglutaminase) are known • Elimination of the environmental trigger leads to a complete resolution of the disease • Permanent sensitivity to gluten
Why is it Important? • If untreated it poses long-term adverse health consequences including: • Malabsorption • Anemia • Poor growth • Osteopenia • Intestinal lymphoma • Nutritional Deficiencies • Iron, zinc, calcium, Vitamin A, D, E, and K
Occurrence • Healthy Population: 1:133 • First-Degree Relative 1:18 to 1:22 • Second-Degree Relative 1:24 to 1:39 • Incidence- Females more than males
Pathogenesis Necessary Causes Genetics Gluten Gender Infant feeding Infections Microbiome Others Pathogenesis ? Risk Factors Celiac Disease
Pathogenesis • Genetic- multi-factorial, polygenic • HLA DQ2 and DQ8 are most common, but, not the only • Over 90% of patients with CD have the DQ2 • Not diagnostic, 40% of population is DQ2+ • We know it is genetic-familial clustering • 10% risk in first degree relatives • HLA identical siblings-30% • Monozygotic twins 75% • Dizygotic twins-10%
Dietary Factors The Grass Family - (GRAMINEAE) Subfamily Tribe Festucoideae Zizaneae Oryzeae Hordeae Aveneae Festuceaea Chlorideae wild rice rice wheat oat finger millet teff (ragi) rye barley
The Celiac Iceberg Symptomatic Celiac Disease Manifest mucosal lesion Silent Celiac Disease Normal mucosa Latent Celiac Disease Genetic susceptibility: - DQ2, DQ8 Positive serology
Clinical Manifestations • Gastrointestinal Symptoms (“Classic”) • Chronic or recurrent diarrhea • Abdominal distention • Abdominal pain • Vomiting • Anorexia • Failure to thrive or weight loss • Constipation • Irritability
Non-Gastrointestinal Manifestations • Dermatitis Herpetiformis • Dental enamel hypoplasia • Osteopenia • Osteoporosis • Short Stature • Delayed Puberty • Infertility • Elevated transaminases • Arthritis • Neurological • Epilepsy • Ataxia • Neuropathy • Dementia • Iron Deficiency Anemia
Dermatitis Herpetiformis • Erythematous macule > urticarial papule > tense vesicles • Severe pruritus • Symmetric distribution • 90% no GI symptoms • 75% villous atrophy Garioch JJ, et al. Br J Dermatol. 1994;131:822-6. Fry L. Baillieres Clin Gastroenterol. 1995;9:371-93. Reunala T, et al. Br J Dermatol. 1997;136-315-8.
Zelnick et al. Pediatrics. 2004. Neurological and Behavioral Problems
Asymptomatic • Treatment with a gluten-free diet is recommended for asymptomatic children with proven intestinal changes. • Asymptomatic patients at risk of osteopenia/osteoporosis • Screening in asymptomatic patients: • Type 1 diabetes 10-20% • Selective IgA deficiency 5% • Down syndrome 5% • Turner syndrome 5% • Williams syndrome 5% • A first degree relative with CD 10%
Serological Tests Role of serological tests: • Identify symptomatic individuals who need a biopsy • Screening of asymptomatic “at risk” individuals • Supportive evidence for the diagnosis • Monitoring dietary compliance
Serum IgA Level • IgA deficient individuals may have false negative EMA-IgA & TTG-IgA • Screen by checking total IgA level or including an IgG based assay EMA-IgG and TTG-IgG) • Approximately 6 % of Celiac Disease patients have IgA deficiency
Antigliadin Antibodies • Antibodies (IgG and IgA) to the gluten protein in wheat, rye and barley • Advantages • Relatively cheap & easy to perform • Improved sensitivity & specificity in young children • Disadvantages • Poor sensitivity and specificity overall
Deamidated Gliadin Antibody • Most recent antibody test available • Antibody response to deamidatedgliadin in patients with Celiac Disease seems to be more intense than the antibody response to native gluten (AGA). • Recent studies have shown that anti-TTG still performs better, and it is currently significantly less costly than anti-DGP testing.
Tissue Transglutaminase - TTG • IgA based antibody against tissue transglutaminase (Celiac Disease autoantigen) • Typically the screening test of choice due to availability and cost • Advantages • High sensitivity and specificity (human TTG) • Non operator dependent (ELISA/RIA) • Relatively cheap • Disadvantages • False negative in young children • Only slightly less specific than EMA
Endomysial Antibody - EMA • Advantages • High sensitivity and specificity • Found in 90-100% of celiac patients • Found in 60-70% of dermatitis herpetiformis patients • Disadvantages • False negatives in young children • Operator dependent • Expensive & time consuming
HLA Tests • Potential role for DQ2/DQ8 • Asymptomatic relatives • Trisomy 21, Turner & Williams syndrome • Type 1 diabetes • Diagnostic dilemmas • TTG +, EMA -, Bx -, Symptoms +
Role of Endoscopy • To obtain a small intestinal biopsy for histologic analysis to establish the diagnosis of CD Normal Appearing Scalloping Nodularity
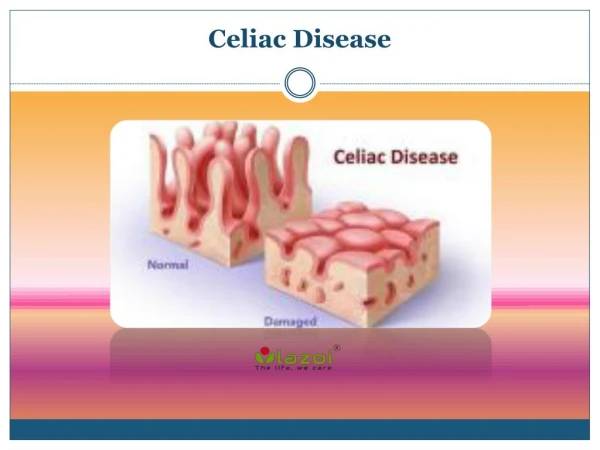
Histologic abnormalities associated with CD are characteristic, but not completely specific. Classically, small intestinal mucosal surface is flattened with absence or marked blunting of intestinal villi Total absorptive surface area is greatly reduced There are typically an increased number of inflammatory cells present in the lamina propria (plasma cells, CD4 cells) Intestinal Histopathology
Treatment • Only treatment for Celiac Disease is a gluten-free diet (GFD) • Strict, lifelong diet • Avoid: • Wheat • Rye • Barley • Oats?
Why is Adherence Important? • Good evidence to suggest that when children with symptomatic celiac disease adhere to a GFD it results in resolution of GI symptoms, improved growth in height and weight, and normalization of hematological and biochemical parameters. • Celiac disease is associated with an overall increased risk of mortality in adults which is primarily the result of GI malignancies. When CD is diagnosed in childhood and GFD is initiated, there appears to be no increased cancer risk and reduced risk of other autoimmune diseases.
Summary • Celiac Disease is a common, subtle enteropathy with variable presentation. • Active, appropriate screening is needed to avoid long-term complications of untreated CD. • Life long adherence to the diet is important