Download
1 / 20
420 likes | 927 Views
Role of Candesartan. Antagonist: AT 1 receptor interaction. Losartan. Candesartan. R. R. Rapid dissociation. Slow dissociation. Surmountable antagonism. Lower affinity. High affinity. Insurmountable antagonism. Re-association and prolonged antagonism.

E N D
Antagonist: AT1 receptor interaction Losartan Candesartan R R Rapiddissociation Slowdissociation Surmountableantagonism Lower affinity High affinity Insurmountableantagonism Re-association and prolonged antagonism Morsing P, Vauquelin G. Cell Biochem Biophys 2001; 35(1): 89–102.
Chemical Structures of Angiotensin II Receptor Blockers O CI N N CO2H N CO2H N N N N N N N N N N N N N N N NH NH NH NH NH EXP 3174 Valsartan N N OCH2CH3 N N O CO2H Irbesartan Candesartan CH3 H3C C N OH CO2H N Olmesartan
Insurmountable and Surmountable Antagonism: Relation to Duration of Binding 100 candesartan 80 telmisartan olmesartan EXP 3174 60 Insurmountability (%) valsartan 40 irbesartan 20 losartan 0 0 20 40 60 80 100 120 Dissociation t1/2 Van Liefde et al 2009
Candesartan: selected properties Easthope SE, Jarvis B. Drugs 2002; 62: 1253–1287. Specific blockade of the effects of angiotensin II through selective AT1 receptor blockade Induces dose-dependent reduction in DBP response to exogenous angiotensin II The antihypertensive effect persists for more than 24 hours; this long duration of action appears to be related to a slow dissociation rate from the AT1 receptor Has placebo-like tolerability in hypertension clinical trials
The TROPHY Study Placebo Placebo Life style counseling QualificationPeriod Life style counseling Placebo Candesartan (16mg) Years 3 and 4 Years 1 and 2 At Visit 1: < 159/85-99 mm Hg or 130-159/ < 99 mm Hg Avg. of 3 Visits: < 139/85-89 mm Hg or 130-139/ < 89 mm Hg
TROPHY Study: ARB in Prehypertension 100 80 Placebo 60 Cumulative Incidence (%) 40 Candesartan 20 0 0 1 2 3 4 StudyYear Julius NEJM 2006; 354 : 1685-97
120 Losartan 30 nM (n=11) Vehicle (n=37) 100 EXP-3174 1 nM (n=9) 80 Irbesartan 50 nM (n=9) Candesartan 1 nM (n=12) 60 40 20 0 Long-lasting AT1-receptor blockade in isolated rat vessels Response to angiotensin II (%) -30 0 30 60 90 120 150 180 Antagonist Time (min) Morsing P, et al. Hypertension 1999; 33(6): 1406–1413.
Meta-analysis based on USA New Drug Application evaluation reports Losartan Irbesartan Valsartan Candesartan 0 –1 –2 –3 Reduction in DBP(mmHg) –4 –5 –6 –7 –8 –9 –10 Losartan Irbesartan Valsartan Candesartan 0 0 0 0 25 75 80 4 50 150 160 8 75 225 240 12 100 300 320 16 Dose (mg)* * x-axis is extended to the highest recommended dose in the EU at the time of meta-analysis Elmfeldt D, et al. Blood Press 2002; 11: 293–301.
Mean change from baseline to week 8 in SBP Hours after dose 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 0 –2 –4 –6 Losartan (100 mg) –8 p=0.004 Change in SBP (mm Hg) –10 –12 –14 Candesartan(16 mg) –16 –18 Lacourciere Y, Asmar R. Am J Hyper 1999; 12: 1181–1187.
Mean change from baseline to week 8 in DBP Hours after dose 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 0 Losartan (100 mg) –2 –4 –6 Change in DBP (mm Hg) p=0.022 –8 –10 Candesartan(16 mg) –12 Lacourciere Y, Asmar R. Am J Hyper 1999; 12: 1181–1187.
TROUGH 48 hours POST-DOSE DBP SBP DBP SBP 0 0 –4 –4 –8 –8 Mean change from baseline (mm Hg) Mean change from baseline (mm Hg) –12 –12 ** * ** –16 –16 *p<0.001 compared with losartan * **p<0.0001 compared with losartan Candesartan Losartan The CLAIM study:candesartan vs. losartan Bakris G, et al. J Clin Hypertens (Greenwich) 2001; 3(1): 16-21.
Headache Respiratory infection Placebo (n=573) Back pain Candesartan (n=1388) Dizziness Nausea Cough 0 1 2 3 4 5 6 7 8 9 10 11 % of patients reporting adverse events Candesartan: adverse events in hypertension trials Belcher G, et al. J Hum Hyper 1997; 11: S85–S89.
Candesartan: tolerabilityin hypertension trials 5 4 3 Withdrawals due to adverse events (%) 2 1 2.4 1.6 2.2 1.6 0 n=573 Placebo n=311 4 mg n=537 8 mg n=303 16 mg Candesartan Belcher G, et al. J Hum Hyper 1997; 11: S85–S89.
Real Life study: CVD Risk Primary composite endpoint 35 Losartan Candesartan 30 25 20 Cumulative incidence (%) 15 10 5 Adjusted risk reduction 14.4% p=0.0062 Unadjusted risk reduction 20.6% p<0.0001 0 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 Time (months) Number at risk Los. 95 923 715 526 385 259 183 6771 5812 4548 3913 3188 2591 2090 1738 1458 1169 Can. 78 794 592 436 257 152 7329 6291 4860 4091 3385 2742 2242 1875 1580 1302 1021
Real Lifestudy: Risk of Separate Endpoints A Heart failure B Arrhythmias C Peripheral artery disease Losartan Losartan Losartan 12 12 12 Candesartan Candesartan Candesartan 10 10 10 8 8 8 Cumulative incidence (%) Cumulative incidence (%) 6 6 6 Cumulative incidence (%) 4 4 4 2 2 2 Adjusted risk reduction 35.9% p=0.0004 Adjusted risk reduction 38.8% p=0.0140 Adjusted risk reduction 20.0% p=0.0330 Unadjusted risk reduction 41.9% p<0.0001 0 0 Unadjusted risk reduction 44.1% p=0.0035 Unadjusted risk reduction 26.7% p=0.0029 0 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 Time (months) Time (months) Time (months) Number at risk Number at risk Number at risk Los. Los. 225 126 834 624 460 320 Los. 6771 5932 4696 4087 3376 2788 2273 1907 1619 1331 1063 820 611 456 314 221 126 6771 5902 4666 4057 3347 2761 2252 1887 1602 1317 1044 814 598 439 301 212 115 6771 5909 4666 4053 3337 2745 2235 1874 1591 1300 1041 Can. Can. Can. 179 91 892 677 507 307 878 664 496 301 175 89 7329 6400 4983 4244 3541 2883 2382 2009 1706 1424 1128 7329 6385 4975 4230 3529 2875 2372 1998 1693 1409 1113 90 867 654 488 294 169 7329 6380 4968 4216 3515 2855 2351 1977 1677 1390 1097 D Chronic ischemic heart disease E Myocardial infarction F Stroke 12 12 12 10 10 10 8 8 8 6 6 6 Cumulative incidence (%) Cumulative incidence (%) Cumulative Incidence (%) 4 4 4 2 2 2 Adjusted risk reduction 14.3% p=0.1400 Adjusted risk reduction 7.0% p=0.5600 Adjusted risk reduction 5.2% p=0.6400 0 Unadjusted risk reduction 19.6% p=0.0350 0 Unadjusted risk reduction 15.5% p=0.1800 Unadjusted risk reduction 12.0% p=0.2600 0 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 Time (months) Time (months) Time (months) Number at risk Number at risk Number at risk Los. Los. Los. 798 590 431 297 208 113 6771 5903 4659 4044 3335 2741 2234 1872 1577 1286 1021 822 612 452 312 221 123 819 609 448 307 217 118 6771 5921 4686 4079 3364 2782 2272 1904 1610 1318 1047 6771 5916 4681 4064 3361 2769 2251 1887 1598 1309 1047 Can. Can. Can. 89 854 644 480 290 172 7329 6378 4950 4205 3502 2844 2345 1968 1670 1384 1091 91 89 876 661 494 299 175 877 662 489 295 172 7329 6387 4972 4231 3516 2858 2362 1992 1688 1406 1113 7329 6374 4963 4220 3515 2859 2362 1991 1691 1408 1113
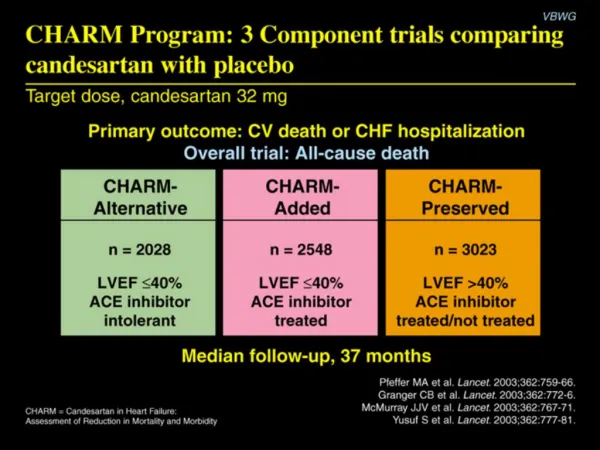
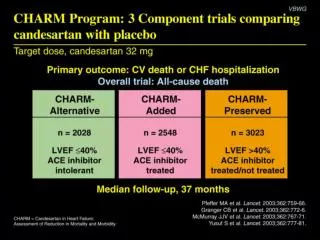
CHARM study programme Three component trials comparing candesartan with placebo in patients with symptomatic heart failure CHARM-preserved CHARM-alternative CHARM- added n=2028 LVEF £40%ACE inhibitor intolerant n=2548 LVEF £40%ACE inhibitor treated n=3025 LVEF >40%ACE inhibitor treated/not treated Primary outcome for each trial: CV death or CHF hospitalisation Primary outcome for overall programme: all-cause death Pfeffer MA, et al. Lancet 2003; 362(9386): 759–766.
CHARM-Added CHARM-Alternative Placebo Placebo Proportion with cardiovascular death or hospital admission for CHF (%) Candesartan Candesartan Proportion with cardiovascular death or hospital admission for CHF (%) 10 HR 0.77 (95% CI 0.67–0.89), p=0.0004Adjusted HR 0.70, p<0.0001 HR 0.85 (95% CI 0.75–0.96), p=0.011Adjusted HR 0.85, p=0.010 yrs CHARM-Preserved CHARM-Overall 50 50 50 50 Placebo 40 40 40 40 Proportion with cardiovascular death or hospital admission for CHF (%) Proportion with cardiovascular death or hospital admission for CHF (%) Placebo Candesartan 30 30 30 30 Candesartan 20 20 20 20 HR 0.89 (95% CI 0.77–1.03), p=0.118Adjusted HR 0.86, p=0.051 HR 0.84 (95% CI 0.77–0.91), p<0.0001Adjusted HR 0.82, p<0.0001 10 10 10 10 0 0 0 0 0 0 0 0 1 1 1 1 2 2 2 2 3 3 3 3 3.5 3.5 3.5 3.5 yrs yrs yrs yrs CV death and CHF hospitalisation in the CHARM studies • Yusuf S, Pfeffer MA, Swedberg K, et al. Lancet 2003; 362(9386): 777–781. • Granger CB, McMurray JJ, Yusuf S, et al. Lancet 2003; 362(9386): 772–776. • McMurray JJ et al, Lancet 2003; 362(9386): 767–771 • Pfeffer MA et al; Lancet 2003; 362(9386): 759–766.
CHARM-Overall: new diagnosis of diabetes 12 10 202 (7.4%) Control Candesartan p=0.020 8 163 (6.0%) 6 Proportion of patients (%) 4 2 0 0 1.0 2.0 3.0 3.5 Time (years) Candesartan 2715 2565 2395 1662 Placebo 2721 2501 2304 1622 Hazard ratio=0.78; 95% CI: 0.64–0.96 Yusuf S, et al. Circulation 2005; 112(1): 48–53.
Comparing Candesartanwith other antihypertensive agents • Adapted from Easthope SE, Jarvis B. Drugs 2002; 62: 1253–1287. • Adapted from McClellan KJ, Goa KL. Drugs 1998; 56: 847–869.