Download
1 / 16
160 likes | 267 Views
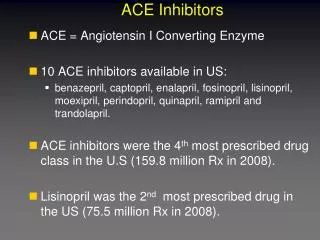
C. Safety of Candesartan in CHF When Added to Evidence-based Doses of ACE Inhibitors. James W. Hainer, MD, MPH AstraZeneca. 59. Client fax 2-7-05. CHARM Protocol—Monitoring Directives for Blood Pressure, Creatinine, and Potassium. At baseline Within 2 wks of dose adjustment

E N D
C Safety of Candesartan in CHFWhen Added to Evidence-based Doses of ACE Inhibitors James W. Hainer, MD, MPH AstraZeneca
59 Client fax 2-7-05 CHARM Protocol—Monitoring Directives for Blood Pressure, Creatinine, and Potassium • At baseline • Within 2 wks of dose adjustment • At end of dose titration • Annually • At any time in the judgment of theresponsible clinician
C HypotensionCHARM Added 2.7.4 Summ Clin safety T 22, 44; SH-AHS-pooled T 150 † One of the reported causes of death.
59 Discontinuation Due to Hypotension in Important Baseline SubgroupsCHARM Added CSR SH-AHS-0006 App 12.1.9.5.22; SAS pgm: rr_hypo_disc_006 All patients Age ≥ 75 Spiro β-blocker BaselineSBP < 100 n = 1272 1276 245 212 215 222 711 702 54 77
C CSR SH-AHS-pooled; data from section 11.3.6.1, T 175; August 11 pmD2454 Briefing Document T22; T_disk_6mos_eos.doc T99 Renal DysfunctionCHARM Added † Renal function abnormal/aggravated, renal failure acute/aggravated, or renal failure NOS. ‡ One of the reported causes of death.
59 Discontinuation Due to Renal Dysfunction in Important Baseline SubgroupsCHARM Added SAS pgm: rr_renal_disc_006; Client analysis SBP < 100 All patients Age ≥ 75 Diabetes Spiro SCr ≥ 2.0† n = 1272 1276 245 212 54 77 382 376 215 222 20 26 † North American sites.
C 2.7.4 Summ Clin Safety T22, 44; Clin Study Rpt T 150 HyperkalemiaCHARM Added † One of the reported causes of death.
59 CSR SH-AHS-Pooled T 66; T68; 12.1.9.5.22; AZ BD T 22 Discontinuation Due to Hyperkalemia in Important Baseline SubgroupsCHARM Added All patients Age ≥ 75 Diabetes Spiro K+ ≥ 5.0† SCr ≥ 2.0† n = 1272 1276 245 212 382 376 215 222 50 64 20 26 † North American sites.
C Summary of Adverse EventsCHARM Added 2.7.4 Summ Clin safety T 21
10-6 2.7.4 Summ Clin safety T 33 Common Serious Fatal Adverse EventsCHARM Added
Outcomes by β-blocker and Spironolactone Use CHARM Added Table 102, App 12.1.9.4.73,74,77,78 Candesartanbetter Placebobetter 0.5 1 1.5 Hazard ratio (95% CI)
Cumulative Number of Hospital Admissions for Any CauseCHARM Added 3000 Placebo 2500 Candesartan 2000 No. of admissions 1500 1000 500 0 0 50 100 150 200 Week
Rates of Hospital Admission by CauseCHARM Added 1.6 Placebo Candesartan 1.4 1.2 1.0 Admissions/patient/yr 0.8 0.6 0.4 0.2 0 All CV HF Non-CV
All-Cause MortalityCHARM Added 35 Placebo Candesartan 30 25 20 Cumulative risk, % HR = 0.88 (95% CI: 0.77, 1.02) 15 10 5 0 0 6 12 18 24 30 36 42 48 Time, mo
C Safety Findings and ConclusionsCHARM Added • As expected, due to the greater RAAS inhibition, rates of hypotension, abnormal renal function, and hyperkalemia were greater with candesartan • These predictable adverse events did not translate into any increases in all-cause hospitalization and/or mortality as well as sudden death, renal failure, or ventricular fibrillation • Candesartan is safe and generally well-tolerated by patients with CHF receiving evidence-based doses of ACE inhibitors
Risk MinimizationCHARM Added • Warnings/precautions • Hypotension, renal dysfunction, hyperkalemia • Patients/populations at risk • Recommendations for monitoring and reducing risk • Interactions with major societies/treatment guideline committees • Sales force/scientific liaison training • Physician, pharmacists continuing medicaleducation programs • Risks displayed in promotional materials • Patient information brochures and updated websites