Download
1 / 31
310 likes | 623 Views
Muscular Dystrophies. Lhedaven C. Santos R.N. Muscular Dystrophies. Progressive hereditary degenerative diseases of the skeletal muscle Intact spinal motor neurons, muscular nerves, and nerve endings in the presence of severe degenerative changes in muscle fibers General features:

E N D
Muscular Dystrophies Lhedaven C. Santos R.N.
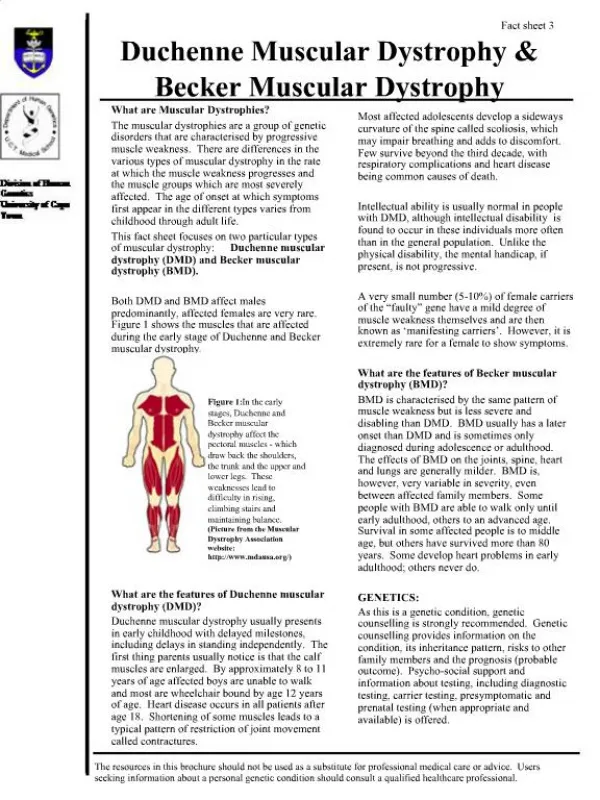
Muscular Dystrophies • Progressive hereditary degenerative diseases of the skeletal muscle • Intact spinal motor neurons, muscular nerves, and nerve endings in the presence of severe degenerative changes in muscle fibers • General features: • symmetrical distribution of weakness and atrophy • intact sensation • preservation of reflexes • heredofamilial • Classified by clinical types, pattern of inheritance and by the abnormal gene or it’s protein product
Etiology • The abnormal gene and the gene product for Duchenne and Becker identified by Kunkel in 1986 • Dystrophin is the protein encoded by the affected gene • Dystrophin absent in Duchenne and structurally abnormal in Becker • Dystrophin in normal skeletal and cardiac muscle is localized in the sarcolemma (cytoplasmic site) and interacts with F-actin of the cytoskeleton (reinforcing structure of muscle cell) • Dystrophin also bound to a complex of sarcolemmal proteins known as dystrophin associated proteins (DAP)
Etiology • Loss of dystrophin leads to disruption of the dystroglycan-protein complex rendering the sarcolemma susceptible to breaks during contraction • These defects are shown to allow ingress of EC fluid and calcium which activate proteases and cause protein degradation • Leakage of CK into serum is then seen
Duchenne MD • Incidence rate 13-33 per 100,000 male births annually • X-linked recessive • 30% of cases represent new mutations • Females can present disease if only one chromosome is present (Turner) or due to inactivation of the normal paternal X chromosome in large proportion of embryonic cells (decreased expression of the normal dystrophin allele)
Clinical findings • Recognized usually in third year of life due to delay in motor milestones or due to frequent falls • Latter sway back and waddling gait (weak gluteus medius) as well as climbing stairs become more affected • Elevated CK may be the first clue
Clinical findings • Muscles mostly affected • early: illiopsoas, quadriceps, gluteal • latter: pretibial, pectoral girdle (serratus, pectorals, latissimus) and upper limbs (biceps, brachioradialis) • Muscles pseudo-hypertrophied • gastronemius, lateral vastus and deltoid • have rubbery feel and are less strong and hypotonic than normals
Clinical findings • Weakness of abdominal and paravertebral muscles - lordotic posture and protuberant abdomen when standing and rounded back when sitting • Weak extensors of the knee and hip - difficult to climb stairs or from a chair • Use of hands to compensate for weakness when rising from sitting position or from floor
Gower’s maneuver • 4 point position • Hands up to thigh alternately
Clinical Findings • Contractures contribute to eventual loss of ambulation • Scoliosis appears due to unequal weakening of paravertebral muscles usually after walking is not possible • As muscle atrophy progresses DTR’s are lost • Bones are thin and demineralized • Can have mild mental retardation • Although smooth muscle is usually spared heart is usually affected
Clinical Findings • Cardiac problems: • Arrhythmias • prominent R waves in right precordial leads and deep Q waves in left precordial and limb leads as result of replacement fibrosis of the basal part of the left ventricular wall • Death is usually 2dary to pulmonary infection and respiratory failure or in some due to cardiac decompensation • No more than 25% of patients survive beyond 25 years
Becker Muscular Dystrophy • Incidence estimated to be 3-6 per 100,000 male births • X-linked disorder • Later onset than Duchenne (mean age 12 years but range 5-45 y/o) • Affects same muscles as Duchenne’s MD • Patient non-ambulatory at 25-30 y/o • Death in 5th decade in most • Less frequent cardiac involvement • Serum CK 25-200 times normal • EMG: fibrillations, positive waves, low amplitude polyphasic MUP
Facioscapulohumeral MD • Slowly progressive or nearly complete arrest • Usually autosomal dominant 4 q35 • Subvariety w/o facial weakness • Onset usually 6-20 y/o • Difficulty raising arms above head and winging of the scapulae first manifestations • Invariably weakness of lower trapezius and sternal part of pectoralis • Deltoids unusually large and strong • Weak orbicularis oculi and oris,zygomaticus
Facioscapulohumeral MD • Eventually atrophy involves sternomastoid, serratus, rhomboid, erector spinae, latissimus and deltoids • Winged and elevated scapulae, prominent clavicles • Popeye arm: upper arm thinner than forearm • Pelvic muscles involved later and milder • Can be asymmetrical • CPK can be normal or mildly elevated • Rare cardiac involvement
Scapular winging • Weak (serratus, lower trapezius, rhomboids) stabilizers of scapula cause winging • Scapular angles can be seen when facing the patient
Facioscapulohumeral MD • Foot drop might be seen • Early in the disease weakness can be asymmetrical • Rare cardiac involvement • CPK normal or slightly elevated
Scapuloperoneal MD • Autosomal dominant, Chromosome 12 • Typically involves muscles of the neck, shoulder, upper arms, anterior tibial and peroneal groups • Onset usually in early or middle adulthood • Walking becomes difficult due to foot drop • Symptoms in arms and shoulders usually seen later • Progression slow in most cases
Limb-girdle MD • Heterogeneous group • Children of both sexes affected • No hypertrophy (besides SCARMD) • Adults can have weakness in either pelvic or shoulder girdle or both, if later onset more benign course • Most commonly heredited as autosomal recessive (2A-2J), • Also AD (1A-1E) forms, AD good prognosis • EMG myopathic, CK normal or only moderately elevated, cardiac involvement infrequent
AD Limb Girdle Dystrophies • LGMD 1 • Onset is varied from 4-38 years • CPK is slightly or moderately increased • Can have flexion contractures of elbows, ankles, and IPJ but non-disabling • Slow progression with long periods of arrest • Normal longevity • Some with facial and cardiac involvement • Includes defects in proteins located in myofibril, cell membrane and EC (collagen proteins)
AR Limb Girdle Dystrophies • LGMD 2 • Affects males and females equally • Shoulder and pelvic girdles affected • Defects in proteins located on cell membranes but also on myofibril+nucleus (calpain 3) • SCARMD (2C-2F)- clinically similar to DMB, from 3-12 y/o onset, CPK 10-100 times normal, hypertrophy and joint contractures, rare cardio involvement • Some have involvement of distal lower extremities (dysferlinopathy)
Emery- Dreifuss Muscular Dystrophy • X-linked, chromosome Xq28 -emerin • Age of onset: childhood- adulthood • Weakness first upper arm and pectoral girdle; later pelvic girdle and distal muscles in Lexts • Early appearance of contractures in elbow flexors, extensors of the neck and posterior calf muscles • No pseudohypertrophy • Usually accompanied by severe cardiomyopathy with variable s/a and a/v conduction defects • Death secondary to cardiac problems although general course is benign in most
Oculopharyngeal Dystrophy • Autosomal dominant; chr 14q11.2-14q13 • Usually late onset (after 45th y/o) • Bilateral ptosis and dysphagia noticed as progressive difficulty in swallowing and change in voice, can progress to cachexia • External ocular muscles, shoulder and pelvic muscles can later become weak • CK and aldolase might be normal • EMG only altered in the affected muscle