Download
1 / 228
2.29k likes | 2.48k Views
The Respiratory System. Function of the lungs. Ventilation (breathing) Gas Exchange T he movement of oxygen and carbon dioxide between lungs and tissues via blood Oxygen utilization The use of oxygen by cells to release energy. The respiratory acinus.

E N D
Function of the lungs • Ventilation (breathing) • Gas Exchange • The movement of oxygen and carbon dioxide between lungs and tissues via blood • Oxygen utilization • The use of oxygen by cells to release energy
The respiratory acinus • Cartilage is present to level of proximal bronchioles • Beyond terminal bronchiole gas exchange occurs • The distal airspaces are kept open by elastic tension in alveolar walls
Lung Volume • Lungs must stay open • Atelectasis = accumulation of pleural fluid which compresses the lung and collapses alveoli • Asthma = spasm of bronchiolar smooth muscle narrows the airway and constricts air flow • Emphysema = insufficient respiratory membrane for gas exchange • Interstitial Fibrosis = an accumulation of fibrous tissue stiffens the lung and prevents free flow of air and also interferes with gas diffusion between blood and alveoli
Lung Volume • Spirometry • Diagnostic procedure that measures lung volumes and capacities and flow rate of air going into and out of the lungs • Lung Diseases have typical spirometry patterns • Generalized Diseases come in two categories • Obstructive and Restrictive • Obstructive = limitation of airflow • Restrictive = limitation of lung expansion
Lung Volume • Forced Vital Capacity (FVC) • A volume measurement • The amount of air expelled from maximum inspiration to maximum expiration • Patient takes the deepest breath possible and blows out as much as possible, no timing involved • Forced Expiratory Volume (FEV1) • Rat measurement; the timed measurement of the amount of air expelled from maximum inspiration in the first second of effect • Patient takes the deepest possible breath and breathes out as hard as possible = amount expelled in first second
Lung Volume • FEV1/FVC = ratio is low in Obstructive disease • Ratio is critical in separating obstructive and restrictive lung disease • In Obstructive disease • The rate of air flowing out of the lungs is slowed • The amount the patient can expel is low • Lung volumes are usually normal
Lung Volume • Restrictive disease • The ratio of airflow to lung volume is usually near normal • Limits both volume and flow rate proportionally • Both Obstructive and Restrictive Disease limits gas exchange • Arterial Oxygen levels are low and Carbon Dioxide levels are high
Effect of pH on ventilation • Normal level of HCO3- = 24 mEq/L • Metabolic acidosis (HCO3- < 24) will + ventilation • Metabolic alkalosis (HCO3- >24) will – ventilation • Kidney regulates HCO3- • Normal level of CO2 = 40 mmHg • Respiratory acidosis (CO2 > 40) will + ventilation • Respiratory alkalosis (CO2 < 40) will – ventilation • Lung regulates CO2
Static Lung Volumes • Tidal Volume (500ml) • amount of air moved in or out each breath • Inspiratory Reserve Volume (3000ml) • maximum vol. one can inspire above normal inspiration • Expiratory Reserve Volume (1100ml) • maximum vol. one can expire below normal expiration • Residual Volume (1200 ml) • volume of air left in the lungs after maximum expiratory effort
Static Lung Capacities • Functional residual capacity (RV+ERV) • vol. of air left in the lungs after a normal expir., balance point of lung recoil & chest wall forces • Inspiratory capacity (TV+IRV) • max. vol. one can inspire during an insp effort • Vital capacity (IRV+TV+ERV) • max. vol. one can exchange in a resp. cycle = max exhaled volume • Total lung capacity (IRV+TV+ERV+RV) • the air in the lungs at full inflation
Patterns of Breathing • Eupnea • normal breathing (12-17 B/min, 500-600 ml/B) • Hyperpnea • pulmonary ventilation matching metabolic demand • Hyperventilation ( CO2) • pulmonary ventilation > metabolic demand • Hypoventilation ( CO2) • pulmonary ventilation < metabolic demand • Hypoperfusion • blood flow to alveoli< metabolic demand
Patterns of breathing (cont.) • Tachypnea • frequency of respiratory rate • Apnea • Absense of breathing. e.g. Sleep apnea • Dyspnea • Difficult or labored breathing • Orthopnea • Dyspnea when recumbent, relieved when upright. e.g. congestive heart failure, asthma, lung failure
General Signs and Symptoms of Respiratory Disease • Hypoxia : Decreased levels of oxygen in the tissues • Hypoxemia : Decreased levels of oxygen in arterial blood • Hypercapnia : Increased levels of CO2 in the blood • Hypocapnia : Decreased levels of CO2 in the blood • Cyanosis : Bluish discoloration of skin and mucous membranes due to poor oxygenation of the blood • Hemoptysis : Blood in the sputum
General Signs and Symptoms of Respiratory Disease • Cough • Productive cough = raising fluid to the pharynx • Expectoration = spitting • Non-productive cough or hacking • Dyspnea • Shortness of breath • Airway obstruction • Decreased compliance • Cyanosis • Large quantities of unoxygenated blood
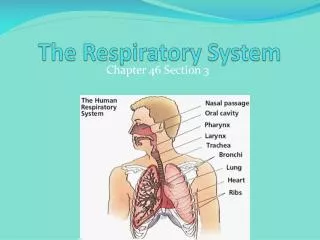
Areas Involved in Respiratory Tract Infections • Upper respiratory tract • Nose, sinuses, pharynx, epiglottis, and larynx • Filters, warms, moisturizes and channels air • Lower respiratory tract • Trachea, bronchi, lungs and pleurae • Oxygenate blood and collects and discharges carbon dioxide, produced by energy metabolism
Upper respiratory tract Infections The common cold The most common viral pathogens for the “common cold” are rhinovirus, parainfluenza virus, respiratory syncytial virus, adenovirus and coronavirus. • These viruses tend to have seasonal variations in their peak incidence. • They gain entry to the body through the nasal mucosa and the surfaces of the eye. They are readily spread from person to person via respiratory secretions. • Manifestations of the common cold include: • Rhinitis:Inflammation of the nasal mucosa • Sinusitis:Inflammation of the sinus mucosa • Pharyngitis:Inflammation of the pharynx and throat • Headache • Nasal discharge and congestion
Upper respiratory tract Infections Influenza • Influenza is a viral infection that can affect the upper or lower respiratory tract. • Three distinct forms of influenza virus have been identified: A, B and C, of these three variants, type A is the most common and causes the most serious illness. • The influenza virus is a highly transmissible respiratory pathogen. • Because the organism has a high tendency for genetic mutation, new variants of the virus are constantly arising in different places around the world. Serious pandemics (spread of infection across a large region) of influenza are seen every 8 to 10 years as a result of this genetic mutation .
Upper respiratory tract Infections Influenza • Symptoms of influenza infection: • Headache • Fever, chills • Muscle aches • Nasal discharge • Unproductive cough • Sore throat • Influenza infection can cause marked inflammation of the respiratory epithelium leading to acute tissue damage and a loss of ciliated cells that protect the respiratory passages from other organisms. • As a result, influenza infection may lead to co-infection of the respiratory passages with bacteria. • It is also possible for the influenza virus to infect the tissues of the lung itself to cause a viral pneumonia.
Upper respiratory tract Infections Treatment of influenza: Bed rest, fluids, warmth Antiviral drugs Influenza vaccine : Provides protection against certain A and B influenza strains that are expected to be prevalent in a certain year. The vaccine must be updated and administered yearly to be effective but will not be effective against influenza strains not included in the vaccine. The influenza vaccine is particularly indicated in elderly people, in individuals weakened by other disease and in health-care workers Influenza
Upper respiratory tract Infections Influenza Drugs for Treating Influenza: • Amantidine • Used orally or by aerosol administration • Effective only against type A influenza • Inhibits viral fusion, assembly and release from the infected host cell • Neuraminidase inhibitors (Zanamavir, Oseltamivir) • New drugs that can be used by inhalation (Zanamavir) or orally (Oseltamivir) • Effective against both type A and B influenza • Inhibits the activity of viral neuraminidase enzyme that is necessary for spread of the influenza virus
Types of Influenza Vaccinations • Trivalent inactivated influenza vaccine (TIIV) • Developed in the 1940s • Administered by injection • Live, attenuated influenza vaccine (LAIV) • Approved for use in 2003 • Administered intranasally
Lower respiratory tract Infections Pneumonia • Pneumonia is a condition that involves inflammation of lower lung structures such as the alveoli or interstitial spaces. • It may be caused by bacteria or viruses such as pneumocystiscarinii. • The prevalence and severity of pneumonia have been heightened in recent years due to the emergence of HIV as well as antibiotic resistance. • Pneumonia may be classified according to the pathogen that is responsible for the infection. • There tend to be distinct organisms that cause pneumonia in the hospital setting vs. the community setting.
Lower respiratory tract Infections Pneumonia • Pathology: • Alveolar • Bronchopneumonia (Streptococcus pneumoniae, Haemophilus influenza, Staphylococcus aureus) • Lobar (Streptococcus pneumoniae) • Interstitial (Influenza virus, Mycoplasmapneumoniae) • Pathogenesis: • Inhalation of air droplets • Aspiration of infected secretions or objects • Hematogenous spread - causing infections away from the original site
Bronchopneumonia vs. Lobar Pneumonia Bronchopneumonia • Acute Inflammation in the walls of the bronchioles Lobar Pneumonia • Lobar pneumonia is a form of pneumonia that affects a large and continuous area of the lobe of a lung
Bronchopneumonia Suppurative (pus) inflammation of lung tissue caused by Staph, Strep, Pneumo & H. influenza Usually bilateral Lower lobes common, but can occur anywhere Complications: Abscess Empyema (is a collection of pus in the space between the lung and the inner surface of the chest wall (pleural space). Dissemination
Lower respiratory tract Infections Pneumonia Individuals Most at Risk for Pneumonia • Elderly • Those with viral infection • Chronically ill • AIDS or immunosuppressed patients • Smokers • Patients with chronic respiratory disease e.g. bronchial asthma.
Potential Pathogens • Typical • Streptococcus pneumoniae • Hemophilusinfluenzae • Mycobacterium catarrhalis • Klebsiellapneumoniae • Atypical • Chlamydiapneumoniae • Legionellapneumophila • Mycoplasmapneumoniae.
Lobar Pneumonia Fibrinosuppurativeconsolidation – whole lobe Rare due to antibiotic treatment. ~95% - Strep pneumoniae The course runs in four stages: Congestion. Red Hepatization – Looks like the liver Gray Hepatizaiton Resolution Lower respiratory tract Infections Pneumonia
Lower respiratory tract Infections Pneumonia • Red hepatisation: (consolidation) describes lung tissue with confluent acute exudation, containing neutrophils and red cells, giving a red, firm, liver-like gross appearance. • Grey hepatisation: follows, as the red cells disintegrate and the remaining fibrinosuppurativeexudate persists, giving a grey-brown appearance. • Resolution: is the favourable final stage in which consolidated exudate undergoes enzymatic and cellular degradation and clearance; normal structure is restored.
Lobar pneumonia: whole lobe(s) involved grey hepatization Lobar pneumonia
Lower respiratory tract Infections Pneumonia A second classification scheme for pneumonia is based on the specific structures of the lung that the organisms infect and includes typical and atypical pneumonia. Typical pneumonia • Usually bacterial in origin. • Organisms replicate in the spaces of the alveoli. Manifestations: • Inflammation and fluid accumulation are seen in the alveoli. • White cell infiltration and exudation can been seen on chest radiographs. • High fever, chest pain, chills, and malaise are present. • Purulent sputum is present. • Some degree of hypoxemia is present.
Lower respiratory tract Infections Pneumonia Atypical pneumonia • Usually viral in origin. • Organisms replicate in the spaces around the alveoli. Manifestations: • Milder symptoms than typical pneumonia. • Lack of white cell infiltration in alveoli. • Lack of fluid accumulation in the alveoli. • Not usually evident on radiographs. • May make the patient susceptible to bacterial pneumonia.
Lower respiratory tract Infections Pneumonia Treatment of pneumonia: • Antibiotics if bacterial in origin. The health-care provider should consider the possibility that antibiotic-resistant organisms are present. • Oxygen therapy for hypoxemia. • A vaccine for pneumococcal pneumonia is currently available and highly effective. This vaccine should be considered in high-risk individuals.
Lower respiratory tract Infections Abscess • An abscess is a complication of severe pneumonia, most typically from virulent organisms such as S. aureus. • Abscesses are complications of aspiration, where they appear more frequently in the right posterior lung.
Lung Abscess: Focal suppuration with necrosis of lung tissue Organisms commonly cultured: Staphylococci Streptococci Gram-negative Anaerobes Frequent mixed infections Mechanism: Aspiration Post pneumonic Septic embolism Neoplasms Productive Cough, Fever. Clubbing Complications:Systemic spread, septicemia.