Download
1 / 49
540 likes | 755 Views
Tamara Datsko associate Professor of Pathology, sectional course and forensic medicine. The EPITHELIAL tumors.

E N D
Tamara Datsko associate Professor of Pathology, sectional course and forensic medicine The EPITHELIAL tumors
The appearance of tumors may be associated with various exogenous and endogenous factors, physical and chemical factors, carcinogens, and viruses, and inherited genetic disorders. • Chemical carcinogens include: • Smoking • Asbest • Aniline dyes, aromatic amines • AflatoxinB • Benzol • Polyvinylchloridum Etiology of tumors
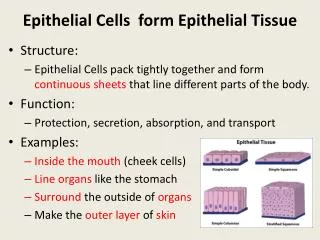
Metaplasia • This is a change from one type differentiated tissue to another , usually of the same broad class but often less well specialised. The change is commonly seen in lining epithelia but occurs also in connective tissues and lining of serous cavities There is frequently an associated hyperplasia. NON NEOPLASTIC PROLIFERATION
MetAplasia • Change from mucus –secreting epithelium to stratified squamous epithelium as in the bronchial irritation associated with smoking NON NEOPLASTIC PROLIFERATION
METAPLASIA • In some cases metaplasia is associated with chronic irritation, but the intimate causes are unknown in most instances. Lack of vitamin A however results in widespread squamous metaplasia of respiratory and salivary epithelium
Dysplasia This means disordered development, as observed in histological sections. The changes consist of increased mitosis, the production of abnormal cells in varying numbers and a tendency to disorder in their arrangement (cellular atypia). Some cases of dysplasia progress to malignancy. The diagram illustrates changes which are common in the uterine cervix
Tumours may be classified in two ways: (1) clinical and (2) histological origin. The tumour is classified according to its morbid anatomy and behaviour. Two main groups are recognised — benign (simple) and malignant.
Although tumours may arise from any tissue in the body, they can be conveniently accommodated in six groups. Mesodermic connective tissues including muscle, bone and cartilage Epethelia Neuroectoderm Haemopoietic tissues Blood and lymph vessels Cells originating from developmental abnormalities In practice, tumours most often take origin from tissues which normally have a rapid turnover of cells and are active in repair — epithelia of skin and mucous membranes, breast and female reproductive organs, connective tissue, bone and haemopoietic cells HISTOLOGICAL ORIGIN
Tumourcellsmaybebroadlydividedintotwotypes: (1) Differentiatedand (2) Undifferentiated. The degree of differentiation roughly corresponds to the character of the neoplasm. Cells of simple tumours arc well differentiated; those of malignant tumours tend to remain undifferentiated, and the more primitive the cells the greater the malignancy
DIFFERENTIATED CELLS (BENIGN TUMOURS) 1. Mimicthestructureoftheirparentorgan.
Lack of differentiation is often termed anaplasia, and anaplastic tumours are highly malignant. There is a spectrum of change in neoplasms from the very slowly growing, highly differentiated simple types to the rapidly growing, undifferentiated malignant examples
PAPILLOMA • Papillomas take origin from an epithelial surface. As the epithelium proliferates it is thrown into folds which become increasingly complex Simple epithelial tumours
Papilloma • The epithelial proliferation is accompanied by a corresponding growth of supporting connective tissue and blood vessels. • Typical examples are found in the skin, e.g. the common wart Simple epithelial tumours
papilloma • In these simple tumours: • The normal arrangement of epithelial cells is maintained, e.g. in skin papillomas the surface cells are squamous and proliferation is confined to the deepest layers. • The relationship of epithelium to connective tissue is normal. • Blood vessels are well formed Simple epithelial tumours
adenoma • Adenomas are derived from the ducts and acini of glands, although the name is also used to cover simple tumours arising in solid epithelial organs. Simple epithelial tumours
adenoma Again the proliferation of epithelium of a gland causes the formation of tubules which ramify and become increasingly compound. The original communication with the parent gland duct or acinus tends to become lost In the case of a hollow viscus, such as the intestine or gall bladder, the adenomatous proliferation, instead of growing down into the subjacent connective tissue, is usually pushed upwards into the lumen of the viscus. — The growth therefore combines the features of a papilloma and an adenoma. The term adenomatous polyp is often applied in such a case. Simple epithelial tumours
adenoma In the type which grows into the subjacent connective tissue, the constant budding of the epithelium results in new acini which become nipped off from the parent acini. In cases in which retention of secretion is marked, a cyst forms and the tumour is then called a cystadenoma which may reach an enormous size, e.g. some cystadenomas of the ovary may be 30-40 cm in diameter, Simple epithelial tumours
adenoma • As in a hollow viscus, the proliferating epithelium may be heaped to form papillomas and the tumour then becomes a papillary cystadenoma. • In some organs the supporting connective tissue of the adenoma is a prominent component of the tumour. This is commonly seen in the BREAST, and the name FIBROADENOMA is used. Depending on the distribution of the fibrous tissue the histological appearances are variable.
Carcinoma in situ (intraepithelial neoplasia) This represents an intermediate stage in the production of a cancer. All the cytological features of malignancy are present, but the cells have not invaded the surrounding tissues. It is frequently found in the cervix uteri at the junction of ecto and endocervix. These premalignant conditions may revert to normal, but most commonly they become truly malignant and invade the surrounding tissues. The determining factors are unknown. The concept of progressive premalignant proliferation applies equally in other organs (e.g. stomach, bowel, bronchus, etc.).
carcinoma • The generic term for a malignant epithelial tumour is CARCINOMA (Greek: Karkinos, a crab). This refers to the irregular jagged shape often assumed. It is due to the local spread of carcinoma
An important principle is that these permeating tumour cells take the line of least physical resistance
The following diagram illustrates the basic mechanisms of cancer cell invasion
LYMPHATIC SPREAD • By definition, all carcinomas spread primarily into the adjacent tissues, and after a varying period, metastasis to more distant structures occurs in the following ways: • LYMPHATIC SPREAD • This is the commonest mode of spread. The carcinoma cells easily invade lymphatic channels from the tissue spaces.
LYMPHATIC SPREAD Groupsofcellsformemboliinthelymphstreamandarecarriedtothenearestnode. Theemboliappearfirstinthecorticalsinus, andthenprogressivelyinvadethetissuesofthenode. Eventuallytheyreachthemedullaandgrowintotheefferentchannelandproducemetastasesinothernodes. Invadednodesareenlarged, firmandwhite. Theseemboliaremicroscopicandcanescapenoticeatoperation. Theyaccountforrecurrenceofgrowthinmanycases. Growthofcarcinomacellsin a noderesultsinocclusionofafferentandefferentchannels. Lymphflowisthusdivertedandthishastwoeffects:
Although lymphatic embolism is of major practical importance , tumour cell may also grow along lymphatic channels in continuous in continuous solid columns lymphatic permeation
Blood spread (venous) Via venules • The entry of malignant cells into the blood is via invasion of venules and by lymphatic embolism througt the thoracic duct into the subclavian vein.
Via larger viens • Occasionally tumour thrombus is propagated from venules into larger veins. This is classically seen in renal carcinoma
Lager veins maym suffer compression effects in 2 ways: • 1. Compression by tumor vein may ultimately by obliterated • 2. Lumen reduced by growth of fibrous tissue stimulated by the neoplasm.
Destination of emboli • This depends on the vessel invaded.
RETROGRADE VENOUS SPREAD Asinlymphatics, growthoftumourwithin a veinmaycausereversalofbloodflow. Inaddition, reversalofflowisapttohappenincertainareasofthebodywhereveinsform a richplexusandaredeficientinvalves, e.g. inthepelvisandaroundvertebrae. Changesinintraabdominalandintrathoracicpressureseasilyinducechangesinbloodflowinthesechannels. Itisforthisreasonthatsecondarytumoursarerelativelycommoninvertebralbodies.
FATE of CARCINOMATOUS EMBOLI SEED and SOIL ANALOGY Thedistributionofcarcinomatousemboliisdeterminedinpartbyanatomy, butmanycomplexfactorsbothinthe'seed' (thecancercell) andthe'soil' (thepotentialmetastaticsite) areatplayintheestablishmentofmetastasesatparticularsites. Theyincludesurfacepropertiesandsecretoryproductsofthecancercellsandreceptorspresentinthecellsandmatrixatthemetastaticsite. Variationinthehost IMMUNE RESPONSE isalsoimportant. Thefollowingfactsemerge:
Size of embolus • Most malignant emboli are tiny and contain few cancer cells. On impaction, the cells commonly die and only an extremely small percentage survive to produce metastases. • Changes at site of embolic impaction • The malignant embolus produces the same changes as any embolus and is treated by the tissues in the same way. Thrombus is deposited on the embolus and platelet and leucocyte functions are stimulated. • The organ affected • Metastatictumoursarecommonin: Lungs.Thisisduetothelargenumberofembolireachingthemincasesofmalignancy. Mostoftheemboliaredestroyedbutsomeareboundtosurvive. Liver.Malignantemboliseemtofindthisorganparticularlyfavourableforfurthergrowth, possiblyduetothehighconcentrationofnutrientmaterialintheportalblood. Metastasesareuncommonin: Spleen. Actively moving tissues: muscle, tendon.Cancercellsmayremainlatentatremotesites (e.g. breastcancercellsinvertebralbonemarrow) andcommenceaggressivegrowthaftermonthsoryears.
GRADING AND STAGING OF CANCER • Two important factors in assessing the prognosis in an individual case of cancer are: • The histological appearance indicating the grade of malignancy. • The size and extent of spread of tumour. • Grading and staging are attempts to quantify these factors. Pathological grading Because this assessment is subjective, it is usual to assign no more than 3 histological grades: well (Grade I), moderately (Grade II) and poorly differentiated (Grade III). Clinico-Pathological staging This is well exemplified in Hodgkin's disease where numerical staging has proved very useful. TNM staging is widely used: T 0-3 indicates local tumour spread, N 0-1 indicates lymph node metastases and M 0-1 distant metastases.
VIA SEROUS SACS • This is an important and frequent route of spread in the peritoneal and pleural cavities. It also takes place in the pericardial sac
As malignant cells sink in peritoneal cavity, they will settle in various sites. They cause an inflammatory reaction with fibrin formation. This anchors the cells and also causes adhesions between organs, providing routes for further spread. • An inflammatory reaction can obscure the presence of carcinoma and make diagnosis difficult.
Intra-epithelial spread • This form of spread may occur where carcinoma develops in a gland or its duct, e.g. in the breast. Carcinoma cells spread in the areolar skin. (Paget's disease of the nipple.)
Squamous cell carcinoma • This is commonly found on the skin, especially exposed surfaces, but also develops in other sites covered by stratified squamous epithelium, e.g. lips, tongue, pharynx, oesophagus and vagina. In addition, it may occur on surfaces covered by glandular type epithelium through metaplastic transformation as in the bronchus, gall bladder and uterine cervix
Histologically, it is composed of irregular strands and columns of invading epithelium which infiltrate the subjacent connective tissue. If well differentiated, the central cells of the invading masses show conversion into eosinophilic keratinised squames, while the outer layer consists of young basophilic cells. In cross-section, the appearance is typical.
The usual features of malignancy — variation in size and shape of cell accompanied by frequent mitotic activity — are present. • Squamous cell carcinoma of skin is usually cornified and slowly growing. Metastasis to the local lymph nodes tends to occur relatively late. • In tumours arising in mucous membranes, growth is more rapid, cornification is inconspicuous and, due to the rich lymphatic drainage, metastasis to lymph nodes occurs early.
Basal cell carcinoma (Rodent ulcer) Thistumourmayariseinanypartoftheskinbutismostcommonintheface, neartheeyesandnose. First stage Itstartsas a flattenedpapillomawhichslowlyenlargesovermonthsorperhaps a yearortwo. Second stage Thesurfacebreaksdownand a shallow, raggedulcerwithpearlyedgesisformed.
Usuallythemalignanttissuespreadsslowlybutprogressively, mainlyin a lateraldirection. Itiscomposedofcellsresemblingthoseofthebasallayeroftheskinfromwhichittakesoriginandhas a characteristichistologicalappearance.
CARCINOMA of GLANDULAR ORGANS • These may take origin from gland acini, ducts or the glandular epithelium of mucous surfaces. The anatomical structure varies.
Occasionaly a carcinoma will produce large quantities of mucus and merit the term mucoid carcinoma. The alveoli may be filled with mucus in which only a few carcinoma cell persist, the cell appearing to dissolve in the mucus. They are commonest in organs normally containing large numbers of mucus-secreting cell, e.g. large intestine, stomach, etc.
These tumours are grouped under the the descriptive term sarcoma, from the Greek sarcoma meaning “Fresh” Sarcomas are less common that carcinomas/ Next to leukaemia, they are the most common malignant tumours in children and young adults. In older age groups, 90% of malignant tumours are carcinomas. Unlike the sinuous infiltrating carcinoma, sarcomas are large fleshy tumours. Arising from and within connective tissues means that infiltration between normal cells advance on a broad front destroing and replacing normal cell. On naked eye assessment these appearances give a false impression and surgical 'shelling out' procedures are almost inevitably followed by local recurrence due to microscopic aggregates of malignant cells remaining in the tumour bed