Download
1 / 63
630 likes | 1.22k Views
Drug Medi -Cal- Organized Delivery System (DMC-ODS) QUALITY ASSURANCE (QA) REQUIREMENTS Phase B. Presented by California Institute for Behavioral Health Solutions. Prepared by Stan Taubman, PhD, LCSW- September 19, 2017. A THREE PHASE TRAINING SERIES. Phase A

E N D
Drug Medi-Cal-Organized Delivery System(DMC-ODS)QUALITY ASSURANCE (QA) REQUIREMENTSPhase B Presented by California Institute for Behavioral Health Solutions Prepared by Stan Taubman, PhD, LCSW- September 19, 2017
A THREE PHASETRAINING SERIES Phase A • Introduction to 42 CFR Part 438 Quality Improvement (QI) requirements. • Addressing QI requirements in a County plan. Phase B • Practical implementation of organizational structure and operation of the QI Committee (QIC). Phase C • Practical implementation of the QI Program in general. • Developing quality standards, analyses, reports, formulating recommendations based on findings, implications for clinical documentation, reducing audit disallowances and other related issues.
Learning Objectives • Quality Improvement Committee (QIC) CONTEXT: Clarify the primary purpose of a QIC in the context of an Organized Delivery System. • QIC STRUCTURE: Identify at least 3 options for the structure, process and function of a QIC capable of accomplishing its primary purpose. • QIC CONTENT: Identify at least 5 issues that a QIC is required to address, and how they relate to its primary purpose. 4. Identify at least 5 databases relevant to QIC monitoring duties. • Identify at least 3 differences between DMC-ODS requirements and Specialty Mental Health (MH) requirements. 6. Identify issues for Phase C training sessions.
THE QUALITY IMPROVEMENT COMMITTEE (QIC) IN ITS ORGANIZATIONAL CONTEXT
ENTITLEMENT • Medi-Cal (MC) establishes entitlements. • MC beneficiaries are entitled to services that are • Medically Necessary, • Accessible, and • Meet Quality Standards
DMC-ODS OBLIGATIONS • DMC-ODS is obligated to meet the substance related entitlements of all MC beneficiaries in its county who seek services. • whether or not its Medi-Cal funds have been depleted in any given year. • This obligation applies to the DMC-ODS, not necessarily to each of its providers.
Quality Improvement Program’s(QIP) PRIMARY PURPOSE A Quality Improvement Program’s (QIP) primary function is to assist DMC-ODS administration in meeting its obligations to beneficiaries for access to services and quality of care.
5 Mandated QIC Functions • recommend policy decisions • review and evaluate the results of QI activities • institute needed QI actions • ensure follow-up of QI process • document QI committee minutes regarding decisions and actions taken Source: DHCS Special Terms and Conditions, Item 156 (b).
WHILE MEETING ITS PRIMARY PURPOSE, A COUNTY’S QI PROGRAM CAN… • promote organizational development (e.g., efficiency, productivity, interagency relations...) • promote quality of clinical practices (e.g., accurate diagnosis, fidelity to evidence based practice methods, treatment plans that are individualized and change when client needs & wishes change...) • improve client outcomes • promote / maintain credibility in the community • minimize legal liabilities (e.g., avoid malpractice suits, prevail if malpractice suits are brought...) • maintain licensure/certifications
PRO FORMA IMPLEMENTATION • Focusing on seeing that every “i” is dotted and every “t” is crossed • Meeting “the letter of the law” without addressing “the spirit of the law” or substance • Striving primarily to show that QI work was done as required by outside agencies
CONSEQUENCES OF PRO FORMA IMPLEMENTATION • The QI Committee and QI staff will have little credibility and little influence in the organization beyond dotting i’s and crossing t’s. • The QI Committee and QI staff will have marginal credibility with external auditors. • Cost/benefit ratio of the QI effort is limited.
WHAT DOES THE QIC NEEDTO BE EFFECTIVE? • backing by an Executive Director committed to accessibility and quality of services • willingness to respectfully speak truth to power within the agency • positive relationships with operations chiefs and middle managers who need to be persuaded to act on QIC findings and recommendations
QIC STRUCTURE What will be the composition and authority of your county’s QIC?
QIP REQUIREMENTS “Describe the County’s Quality Management and Quality Improvement Programs.” - From STC Attachment Z, PART II: Sec. 12 Quality Assurance The description must include…
QIP REQUIREMENTS (cont’d) “…a description of the Quality Improvement (QI) Committee (or integration of DMC-ODS responsibilities into the existing MHP QI Committee).” FOR EXAMPLE… • Composition: Who will be “ex officio” QIC members? • Leadership: Which member will be the Chairperson? • Authority Relations: To whom does the Chairperson report? • Scheduling: How often will the QIC meet?
QIP REQUIREMENTS “…a description of the Quality Improvement (QI) Committee (or integration of DMC-ODS responsibilities into the existing MHP QI Committee).” FOR EXAMPLE… • Will the QIC establish practice standards? • If so, how will they be developed? • What data sources will the QIC review to determine whether or not standards have been met? • To whom will review findings be reported? • Who will develop and evaluate implementation of Corrective Action Plans?
QIC COMPOSITION Who will be “ex officio” members of the QIC? • The County Department Director? • A QI Administrator? • An Operations Chief? • A Finance Director? IT Chief? • A Chief Authorization Reviewer? • Middle Managers at specified service sites? • Administrators of partner agencies?
QIC COMPOSITION Who will be selected members of the QIC? • Service staff representatives? • Consumer representatives? • Family member representatives? • A risk management attorney or County Counsel representative?
The QI Administrator’s Role A Broadly Defined Approach (examples) Tasks: • leading, organizing and managing the QI process • setting the direction for quality activities at the agency • identifying processes that are not working and making them better (clinical practices, accountability, communications…) Responsibilities: • assuring that the agency achieves its mission • assuring that clients achieve their desired outcomes • aligning the agency’s day-to-day work with the requirements of external standards and regulations (accreditation, Medi-Cal, EQRO...) • assuring compliance with agency policies and procedures
The QI Administrator’s Role A More Specifically Defined Approach (examples) Tasks: • conduct chart reviews • create, administer and interpret survey data • write, receive and distribute reports on agency activities Responsibilities: • assure compliance with..... (e.g. policies, procedures…) • assure proper documentation • assure that paperwork is sent through the right channels on time • minimize audit disallowances • assure optimal productivity and revenue generation • assure achievement of agency objectives (if the agency has specific, measurable objectives)
AN EFFECTIVE QIC The effectiveness of QIC members is likely to vary according to: • professional or technical preparation in the practices being monitored • professional or technical preparation in QI procedures, research methodology and data analysis • commitment to continuing education • relationships with operations managers • persuasive “people skills”
WHAT DOES A QIC NEED TO INFLUENCE QUALITY OF CARE? • explicit quality of care standards • some will be provided by EQRO • some will be provided by DHCS • some should be developed within the organization to address its local issues • access to the codified manuals used to establish evidence-based practice methods • authorization to gather information throughout the agency relevant to these standards
KNOWLEDGE BASE OF THE EFFECTIVE QIC MEMBER Knowledge of… • QI processes (e.g., chart reviews, data collection, data management, data analysis, report writing...) • external standards and regulations • organizational structure, dynamics and development • clinical practices (e.g., diagnostic criteria, structured clinical methods, elements of treatment planning, evidence based practices, clinical documentation) • client needs and client rights
BALANCING AUTHORITY AND RESPONSIBILITY What will the QIC or QI Administrator be held responsible for? • Assuring that standards and regulatory requirements are met? • Quality of services? • Staff compliance with agency policies? • Quality of case documentation? • Validity/reliability of QI data & reports? • Fair and effective Corrective Action Plans?
BALANCING AUTHORITY AND RESPONSIBILITY Will the QIC or QI Administrator have the authority to direct the practices of: • Middle Managers? • Practitioners / Service Staff? • Clerical Support Staff? • QIC members? • Anyone? If so…Some Practices? Any Practices?
BALANCING AUTHORITY AND RESPONSIBILITY Will the QIC or QI Administrator have the independent authority to report uncensored findings to: • the Department’s Executive Director? • Middle Managers? • Practitioners / Service Staff? • External Organizations?
QIC CONTENT WHAT MUST BE ADDRESSED BY A COUNTY’S QUALITY IMPROVEMENT COMMITTEE?
7 Mandated QIC Content Issues i. Timeliness of first initial contact to face-to-face appointment ii. Timeliness of services of the first dose of NTP services iii. Access to after-hours care iv. Responsiveness of the beneficiary access line v. Strategies to reduce avoidable hospitalizations vi. Coordination of physical and mental health services with waiver services at the provider level vii. Assessment of the beneficiaries’ experiences viii. Telephone access line and services in the prevalent non-English languages. Source: DHCS Special Terms and Conditions, Item 156 (b).
4 Mandated Types of Data …to be reviewed by QIC at least quarterly i. Number of days to first DMC-ODS service at appropriate level of care after referral ii. Existence of a 24/7 telephone access line with prevalent non- English language(s) iii. Access to DMC-ODS services with translation services in the prevalent non- English language(s) iv. Number, percentage of denied and time period of authorization requests approved or denied Source: DHCS Special Terms and Conditions, Item 156 (c).
What database will your QIC access in order to determine… “…number of days between referral/assessment and first DMC-ODS service/follow-up appointment”?
What database will your QIC access in order to determine… “…the availability of a 24/7 telephone access line with prevalent non-English language(s)”?
What database will your QIC access in order to determine… “…access to translation services in the prevalent non-English language(s)”?
What database will your QIC access in order to determine… “…number and percentage of denied authorization requests and time period of approved or denied authorization requests?”
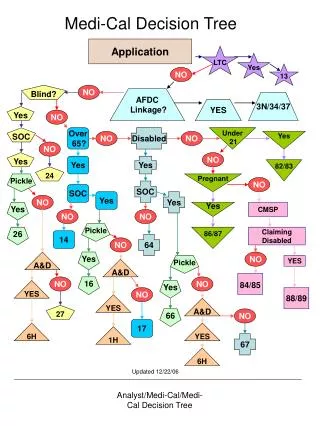
AUTHORIZATION Authorization is a step in “Client Flow”… • Referral • Assessment • Authorization • Placement • Transitions to another level of care Reauthorizations at least every six mos. (annually for NTP services)
AUTHORIZATION AUTHORIZATION IS PART OF A DEPARTMENT’S UTILIZATION MANAGEMENT PROGRAM
UTILIZATION MANAGEMENT “Counties will have a Utilization Management (UM) Program assuring that beneficiaries have appropriate access to substance use disorder services; medical necessity has been established and the beneficiary is at the appropriate ASAM level of care and that the interventions are appropriate for the diagnosis and level of care….” • Source: State DHCS Terms and Conditions, 156(d)
UTILIZATION MANAGEMENT “Counties shall have a documented system for collecting, maintaining and evaluating accessibility to care and waiting list information, including tracking the number of days to first DMC-ODS service at an appropriate level of care following initial request or referral for all DMC- ODS services.” Source: State DHCS Terms and Conditions, 156(d)
MEDICAL NECESSITY • Client has a DSM diagnosis for Substance-Related and Addictive Disorders (other than tobacco related or gambling disorders)… • or is at risk for developing substance use disorder (if under age 21) • Client meets ASAM Criteria for the planned/assigned Level of Care. • Source: State DHCS Special Terms and Conditions 156(d)
MEDICAL NECESSITY DMC ODS Medical Necessity is different than MC Medical Necessity for Specialty Mental Health Services.
…a description of the QIC will address “monitoring of accessibility of services” ACCESSIBILITY IS NOT MERELY AVAILABILITY
ACCESSIBILITY IS NOT MERELY AVAILABILITY An available service is accessible if … • people know about it. • people can get to it (geographical distance, transportation access). • disabled people can enter and use the facility. • staff speak the language of people coming to the program or translation is available. • it’s open when clients can come to it.
ACCESSIBILITY IS NOT MERELY AVAILABILITY (cont’d) “The monitoring of accessibility of services outlined in the Quality Improvement Plan will at a minimum include: • Timeliness of first initial contact to face-to-face appointment • Frequency of follow-up appointments in accordance with individualized treatment plans • Timeliness of services of the first dose of NTP services • Access to after-hours care”
ACCESSIBILITY IS NOT MERELY AVAILABILITY (cont’d) Monitoring of Accessibility (cont.) • Responsiveness of the beneficiary access line • Strategies to reduce avoidable hospitalizations • Coordination of physical and mental health services with waiver services at the provider level • Assessment of the beneficiaries’ experiences, including complaints, grievances and appeals • Telephone access line and services in the prevalent non-English languages.”
STRATEGIES FOR IMPROVING ACCESS (Examples) (1) Add staff positions/hours or contractor services with needed skills in specific geographic areas; (2) Provide services nights and weekends; (3) Allow flex hours, part-time staff, per diem staff, and varied shifts to accommodate staff and client needs for treatment/rehab access; (4) Provide special programs such as loan forgiveness, structured internships to bring in new clinicians to workforce; (5) Use technology to enhance access/training/consultation – such as video conferencing, translation lines/video, telemedicine/psychiatry, therapies to provide services to remote areas and in a variety of languages.
COLLABORATIVE RELATIONSHIPS “The DMC-ODS has developed strongly collaborative programs/relationship with the following providers to enhance access to care and meet a broad array of client ancillary service needs.” Source: California EQRO Draft “Key Components Standards and Review Tool” 6/5/17
COLLABORATIVE RELATIONSHIPS WITH WHOM? • Primary Care Providers/Clinics • Hospitals and/or Emergency Rooms • Mental Health Programs and MH Plans for co-occurring disorders • Child Welfare/Human Services • Educational Systems (K-12, vocational, community college, higher education) • Law Enforcement/Criminal Justice
COLLABORATIVE RELATIONSHIPS WITH WHOM? • Public Health/Health Department • Medi-Cal Health Plans • Community-based Organizations such as meals on wheels, Goodwill, etc. • Faith-based Organizations • Vocational Training and Job Placement • Housing Authority • Self-Help Organizations and Networks
EVIDENCE OF COLLABORATIVE RELATIONSHIPS (examples) • Shared Grants • DMC ODS Planning and implementation reports • DMC ODS initiatives, trainings and outcome reports • MOUs with Organizations • Interagency Referral Protocols • Examples of Joint Initiatives • Committee Minutes • On Site Review Observations/Sessions: Staff and partners report and can give examples of how the DMC ODS integrates services with primary care, substance abuse, criminal justice, schools, etc.
TRACKING NO-SHOWS, CANCELLATIONS, 1ST APPOINTMENTS “DMC-ODS Tracks and Trends No Shows, Cancellations, and ideally First Appointments Offered” Source: California EQRO Key Components Standards and Review Tool Draft 6/5/17
TRACKING NO-SHOWS, CANCELLATIONS, 1ST APPOINTMENTS What to track, by program unit… • Rate of No Shows/Cancellations • What are the barriers to care • Impact of no-shows, cancellations, and barriers on clients • Type of no shows/cancellations (e.g. client initiated or staff cancellations)