Download
1 / 35
530 likes | 1.7k Views
ANAEMIA IN PREGNANCY. ANAEMIA IN PREGNANCY. Commonest medical disorder in pregnancy Out of estimated 160 million deliveries occurring annually in the world, approx 6,00,000 women die from the complications of pregnancy & child birth (W.H.O 1996).

E N D
ANAEMIA IN PREGNANCY • Commonest medical disorder in pregnancy • Out of estimated 160 million deliveries occurring annually in the world, approx 6,00,000 women die from the complications of pregnancy & child birth (W.H.O 1996). • Anaemia is responsible for 40-60% of maternal deaths in developing countries. It also increases perinatal mortality and morbidity rates (W.H.O 1997).
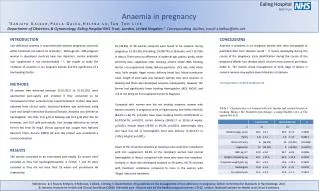
DEFINITION • Anaemia is a condition of low circulating haemoglobin in which haemoglobin concentration has fallen below the threshold lying at two standard deviations below the median value for a healthy matched population. • W.H.O defines anaemia in pregnancy as haemoglobin concentration of less than 11 g/dl and haematocrit of less than 0.33. • The cut-off point suggested by the United States Centers for disease control is 10.5 gm/dl in the second trimester.
ICMR describes four grades of anaemia depending upon the haemoglobin levels as shown: SEVERITY OF ANAEMIA
ERYTHROPOIESIS • Confined to the bone marrow in adults • RBCs are formed through stages of pro-normoblast – normoblast – reticulocytes – mature non-nucleated arithrocyte. • After a life span of 120 days RBCs degenerate and haemoglobin is broken down into haemosiderin and bi-pigment.
ERYTHROPOIESIS (Contd.) • For proper erythropoiesis adequate nutrients are needed: • Minerals: Iron, traces of copper, cobalt and zinc. • Vitamins: Folic Acid, Vitamin B12, Vitamin C, Pyridoxine and riboflavin • Proteins: For synthesis of globin moiety. • Hormones: Androgens and thyroxine.
ERYTHROPOIETIN Erythropoietin is a hormone produced by kidneys (90%) and the liver (10%) • Increased secretion occurs during pregnancy due to placental lactogen and progestrone. • Eryhtropoietin increases red cell volume by stimulating stem cells in the bone marrow. • In addition to common deficiency of folic acid and iron, there is a growing body of evidence to implicate vitamin A in nutritional anaemia.
HAEMATOLOGICAL CHANGES IN PREGNANCY Mean corpuscular haemoglobin = MCH Packed cell volume = PCV Mean corpuscular haemoglobin concentration = MCHC Mean corpuscular volume = MCV Total iron binding capacity = TIBC
PREVALENCE OF ANAEMIA IN PREGNANCY • Overall prevalence – 40% of world’s population • Prevalence of anaemia is 3-4 times higher in developing countries. Average prevalence being 56%. • In industrialized countries approx 18% of women are anaemic during pregnancy. • In India alone the prevalence of anaemia in pregnancy is as high as 88% (W.H.O Global Database 1997).
CLASSIFICATION OF ANAEMIA IN PREGNANCY ACQUIRED: • Iron deficiency anaemia • Anaemia caused by blood loss – Acute (APH) – Chronic (Hook worm infestation, bleeding piles etc.) • Megaloblastic anaemia (Vitamin B12 and folic acid deficiency) • Acquired hemolytic anaemia • Aplastic or hypo-plastic anaemia
CLASSIFICATION (Contd.) HERIDITARY: • Thalassemias • Sickle cell haemoglobinopathies • Other haemoglobinopathies • Hereditary hemolytic anaemias (RBC membrane defects, spherocytosis)
IRON DEFICIENCY ANAEMIA • It is the commonest type of anaemia in pregnancy. • Food iron is made up of two pool • Haem Iron Pool • Non- Haem Iron Pool • Haem Iron Pool includes all food containing iron as haem molecules, such as animal flesh and viscera. Its absorption is 15-30%, but it can increase to 50% in iron deficiency state. Its absorption is usually not affected by inhibitors.
IRON DEFICIENCY ANAEMIA (Contd.) • Non-Haem Iron Pool includes cereals, vegetables, milk and eggs. Its absorption can be increased by enhancers and decreased by inhibitors. • Enhancers of absorption: Haem iron, proteins, meat, ascorbic acid, ferrous iron, gastric acidity, alcohol, low iron stores, increased erythropoietic activity. • Inhibitors of iron absorption: Phytates, calcium, tannins, tea & coffee.
CAUSES OF INCREASED PREVALENCE OF I.D.A • Dietary habits: Consumption of low-bio availability diet • Food Fadism • Defective iron absorption due to intestinal infections, hook worm infestation, amoebiasis, giardiasis. • Increased iron loss: Frequent pregnancies, menorrhagia, hook worm infestation, chronic malaria, excessive sweating, piles. • Repeated and closely spaced pregnancies and prolonged period of lactation.
IRON REQUIREMENT IN PREGNANCY Total iron requirement is 1000 mg. • Fetus and placenta -- 300 mg • ↑ in red cell mass – 500 mg • Basal loss – 200 mg Average requirement is 4-6mg/day. • 2.5 mg/day in early pregnancy • 5.5 mg/day from 20-32 weeks • 6-8 mg/day from 32 weeks onwards
PREVENTION OF IRON DEFICIENCY • Prophylaxis of non-pregnant women – 60 mg of elemental iron daily for 3 months. • Iron supplementation during pregnancy. • Routine iron supplementation is debatable in western countries • It has to be given in non-industrialized countries • W.H.O RECOMMENDATION: Universal oral iron supplementation for pregnant women (60 mg of elemental iron and 250 µg of folic acid) for 6 months in pregnancy and additional of 3 months post-partum where the prevalence is more than 40%.
PREVENTION OF IRON DEFICIENCY (Contd.) • MINISTRY OF HEALTH, GOVT. OF INDIA RECOMMENDATION: 100 mg of elemental iron with 500 µg of folic acid in second half of pregnancy for atleast 100 days. 2 injections of iron dextran (250 mg each) given IMI at 4 weeks interval with TT injection. • Treatment of hook worm infestation • Single albendazole (400 mg) or mebendazole (100 mg x BD x 3 days) • Change in defecation habits and avoidance of walking bare footed.
PREVENTION OF IRON DEFICIENCY (Contd.) • Improvement of dietary habits and improving bio availability of food iron • Iron fortification of food.
EFFECTS OF ANAEMIA ON PREGNANCY • Maternal effects: ANTE NATAL INTRA NATAL POST NATAL Poor weight gain Dysfunctional labour Puerperal Sepsis Preterm labour Haemorrhage & shock Sub-involution Pre-eclampsia Cardiac failure Embolism Abruptio placentae Inter current infections PROM
EFFECTS OF ANAEMIA ON PREGNANCY (Contd.) • Fetal effects: • Risk of pre-maturity • IUGR, LBW, poor apgar score • Depleted iron store in neonates and anaemia in infancy period • High prevalence of failure to thrive and poor intellectual development. • Cardiovascular morbidity and mortality in adult lives.
INVESTIGATIONS • Haemoglobin estimation • Peripheral blood smear – microcytosis, hypochromia anisocytosis, poykilocytosis and target cells • RBC indices – ↓MCV, ↓MCH, ↓MCHC, MCV is the most sensitive indicator • ↓ Serum ferritin – first abnormal laboratory test • ↓ Transferrin saturation – second to be affected • ↑ FEP – third test to become abnormal • ↑ Serum transferrin receptor – best indicator
INVESTIGATIONS (Contd.) • Bone marrow examination – no response to treatment after 4 weeks of therapy • Aplastic anaemia • Diagnosis of kala-azar • Urine examination • Stool examination – for three consecutive days • Other tests – RFT, LFT, TSP A:G, chest x-ray, sputum examination, etc. • For response – haemoglobin and PBS, reticulocyte count
MANAGEMENT OF IRON DEFICIENCY ANAEMIA AIM • To correct iron deficiency • To restore iron reserve • To correct associated complicating factor CHOICE OF THERAPY • Depends on severity of anaemia • Duration of pregnancy • Associated complicating factor
MANAGEMENT (Contd.) GENERAL TREATMENT • Dietary advice • Treatment of associated complicating factor IRON THERAPY • Oral • Parenteral
ORAL IRON THERAPY • For women presents in mid trimester or early third trimester • For treatment more than 180 mg of elemental iron/day is required • To minimize side effects, start with low dose • Treatment is continued till blood picture becomes normal, thereafter maintenance of one tablet daily for 3 months to replenish iron stores
INDICATIONS OF RESPONSE TO THERAPY • Sense of well being • Improved outlook of patient • Increased appetite • ↑ haemoglobin, haematocrit, reticulocytosis within 5-10 days If no significant clinical or haematological improvement within 3 weeks, diagnostic re-evaluation is needed.
INDICATIONS OF RESPONSE TO THERAPY (Contd.) • RATE OF IMPROVEMENT: After a lapse of few days haemoglobin concentration is expected to rise at a rate of 0.7 g/dl/week. • CAUSES OF FAILURE OF ORAL THERAPY • Incorrect diagnosis • Malabsorption syndrome • Presence of chronic infection • Continuous loss of iron • Poor patient compliance • Concomitant folate deficiency.
PARENTRAL IRON THERAPY INDICATIONS: • In tolerance to oral iron • Poor patient compliance • Unpredictable absorption • Patient near term ADVANTAGE • No added advantage over oral iron except for certainty of its administration.
PARENTRAL IRON THERAPY (Contd.) PARENTERAL IRON THERAPY • Intra muscular • Intra venous Two preparations – Iron dextran – IM/IV • Iron sorbitol citrate – IM IRON DEFICIT Elemental iron needed (mg) = (Normal Hb – Patient’s Hb) x Weight (kg) x 2.21 + 1000
PARENTRAL IRON THERAPY (Contd.) Simple method is to give 250 mg elemental iron for each gm of haemoglobin below normal. Another 50 % is to be added to replenish store. Oral Iron should be stopped atleast 24 hrs prior to therapy to avoid toxic reaction. Iron injections are given daily or on alternate day by deep IMI using ‘Z’ technique. I.V. ROUTE • Total dose in fusion (TDI) – Dose calculated by same formula
PRE-REQUISITES FOR TDI: • Correct diagnosis of iron deficiency anaemia. • Adequate supervision in hospital setting. • Facility for management of anaphylactic reaction. Sensitivity test done by 1ml test dose prior to infusion: • If no reaction iron dextran is diluted in normal saline or 5% dextrose and given over 4-6 hrs. • If total dose is more than 2500 mg infusion is given in 2 doses on consecutive days. • Look for reaction – Chest pain, rigor chills, hypotension, dyspnoea, haemolysis & anaphylactic reaction.
INDICATION OF BLOOD TRANSFUSION • Severe anaemia beyond 36 weeks • Refractory anaemia • To correct anaemia due to blood loss • Associated infection
MANAGEMENT DURING LABOUR • Iron and folate therapy for 3 months • Infection if any should be treated energetically • Careful watch for puerperal sepsis, failing lactation; sub involution of uterus and thromboembolism • First stage – Comfortable position • Adequate analgesia • Arrangement for oxygen, • Digitalization maybe required in cardiac failure due to severe anaemia • Antibiotic prophylaxis
MANAGEMENT DURING LABOUR (Contd.) • Second stage – Cut short by forceps application. • Active management of third stage • During puerperium • Adequate rest • Iron and folate therapy for 3 months • Infection if any should be treated energetically • Careful watch for puerperal sepsis, failing lactation; sub involution of uterus and thromboembolism