Download
1 / 1
20 likes | 148 Views
Ealing Hospital NHS Trust Anaemia in pregnancy † Sanjaya Kalkur,Paula Galea,Helena Lo ,Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom. † Corresponding Author, email-s.kalkur@nhs.net. INTRODUCTION

E N D
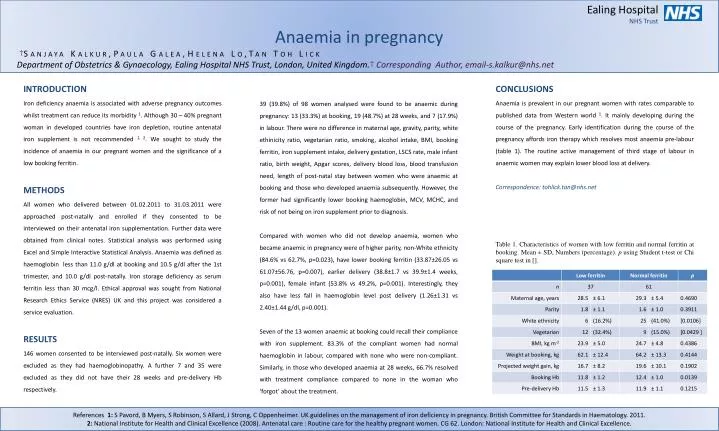
Ealing Hospital NHS Trust Anaemia in pregnancy †Sanjaya Kalkur,Paula Galea,Helena Lo,Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom.†Corresponding Author, email-s.kalkur@nhs.net INTRODUCTION Iron deficiency anaemia is associated with adverse pregnancy outcomes whilst treatment can reduce its morbidity 1. Although 30 – 40% pregnant woman in developed countries have iron depletion, routine antenatal iron supplement is not recommended 1, 2. We sought to study the incidence of anaemia in our pregnant women and the significance of a low booking ferritin. METHODS All women who delivered between 01.02.2011 to 31.03.2011 were approached post-natally and enrolled if they consented to be interviewed on their antenatal iron supplementation. Further data were obtained from clinical notes. Statistical analysis was performed using Excel and Simple Interactive Statistical Analysis. Anaemia was defined as haemoglobin less than 11.0 g/dl at booking and 10.5 g/dl after the 1st trimester, and 10.0 g/dl post-natally. Iron storage deficiency as serum ferritin less than 30 mcg/l. Ethical approval was sought from National Research Ethics Service (NRES) UK and this project was considered a service evaluation. RESULTS 146 women consented to be interviewed post-natally. Six women were excluded as they had haemoglobinopathy. A further 7 and 35 were excluded as they did not have their 28 weeks and pre-delivery Hb respectively. 39 (39.8%) of 98 women analysed were found to be anaemic during pregnancy: 13 (33.3%) at booking, 19 (48.7%) at 28 weeks, and 7 (17.9%) in labour. There were no difference in maternal age, gravity, parity, white ethinicity ratio, vegetarian ratio, smoking, alcohol intake, BMI, booking ferritin, iron supplement intake, delivery gestation, LSCS rate, male infant ratio, birth weight, Apgar scores, delivery blood loss, blood transfusion need, length of post-natal stay between women who were anaemic at booking and those who developed anaemia subsequently. However, the former had significantly lower booking haemoglobin, MCV, MCHC, and risk of not being on iron supplement prior to diagnosis. Compared with women who did not develop anaemia, women who became anaemic in pregnancy were of higher parity, non-White ethnicity (84.6% vs 62.7%, p=0.023), have lower booking ferritin (33.87±26.05 vs 61.07±56.76, p=0.007), earlier delivery (38.8±1.7 vs 39.9±1.4 weeks, p=0.001), female infant (53.8% vs 49.2%, p=0.001). Interestingly, they also have less fall in haemoglobin level post delivery (1.26±1.31 vs 2.40±1.44 g/dl, p=0.001). Seven of the 13 women anaemic at booking could recall their compliance with iron supplement. 83.3% of the compliant women had normal haemoglobin in labour, compared with none who were non-compliant. Similarly, in those who developed anaemia at 28 weeks, 66.7% resolved with treatment compliance compared to none in the woman who ‘forgot’ about the treatment. CONCLUSIONS Anaemia is prevalent in our pregnant women with rates comparable to published data from Western world 1. It mainly developing during the course of the pregnancy. Early identification during the course of the pregnancy affords iron therapy which resolves most anaemia pre-labour (table 1). The routine active management of third stage of labour in anaemic women may explain lower blood loss at delivery. Correspondence: tohlick.tan@nhs.net Table 1. Characteristics of women with low ferritin and normal ferritin at booking. Mean ± SD, Numbers (percentage). p using Student t-test or Chi square test in []. References 1: S Pavord, B Myers, S Robinson, S Allard, J Strong, C Oppenheimer. UK guidelines on the management of iron deficiency in pregnancy. British Committee for Standards in Haematology. 2011. 2: National Institute for Health and Clinical Excellence (2008). Antenatal care : Routine care for the healthy pregnant women. CG 62. London: National Institute for Health and Clinical Excellence.