Download
1 / 28
280 likes | 337 Views
1. Student will be able to list causes and conditions associated with cognitive impairment 2. Student will be able to describe behaviors exhibited with cognitive impairment.

E N D
1. Student will be able to list causes and conditions associated with cognitive impairment 2. Student will be able to describe behaviors exhibited with cognitive impairment. 3. Student will be able to identify and explain therapies/methods to effectively handle residents with challenging behaviors. 4. Student will be able to explain communication strategies and techniques to use with cognitively impaired residents. Cognitive Impairment Dementia/Alzheimer’s DiseaseLesson 21:Objectives
Cognitive Impairment • Temporary or permanent change within the brain that affects a person’s ability to think, reason, and learn ~Temporary Causes: stress, medication, depression, vitamin deficiency, thyroid disease, alcohol, fever, head trauma, brain tumor ~Permanent Causes: severe head trauma, end-stage serious illnesses, brain disease, brain damage at birth, stroke, alcoholism, Alzheimer’s
Cognitive Impairment • Interferes with ability to make decisions • Personality may change • Anger, depression, and irritability are other signs
Aging & the Brain • It is normal for a person to lose some ability to think logically and clearly as he ages. • Elderly residents may lose memory of recent events. • Encourage residents to make lists and to write down names, events, and phone numbers. • Reaction time may slow and it may be harder to find the right word. • Elderly people tend to sleep less. • Dementia is not normal part of aging (common)
Key terms • Depression-prolonged emotional sadness or hopelessness • Delirium-state of severe confusion that occurs suddenly • Delusion- thought or idea with no basis in reality • Dementia- mental decline; loss of mental functioning abilities • Confusion- inability to think, concentrate, reason, or remember clearly
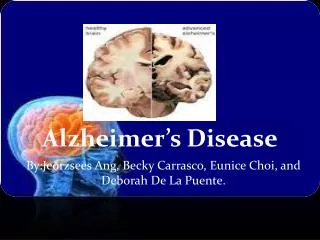
Dementia Alzheimer’s Disease (AD)- progressive, degenerative, irreversible diseased caused by formation of tangled nerve fibers and protein deposits in the brain. • Most common type of dementia • Progression/Life Span varies 2-20yrs • 2-3 million Americans affected • More common in females • Greatest risk after age 65 (40-50’s=early onset) • Family history of AD and Down’s Syndrome
Alzheimer’s Disease Alzheimer’s disease generally progresses in the following stages: • Stage 1 - No impairment • Stage 2 - Very mild decline • Stage 3 - Mild decline • Stage 4 - Moderate decline • Stage 5 - Moderately severe decline • Stage 6 - Severe decline • Stage 7 - Very severe decline • Refer to “Quick Reference” in book (pg. 115)
Alzheimer’s Disease • In stages 5, 6, 7 the resident will need increasing assistance with ADLs, but at all times residents should be encouraged to do what they can for themselves. AD residents will do best if they keep their minds and bodies active for as long as possible.
Cognitive Impairment/Dementia Over stimulation often leads to behaviors ~Common Behaviors: agitation, wandering & pacing, hallucinations/delusions, sundowning, catastrophic reactions, repetitive phrasing (perseverate), violence/aggression, disruptive, paranoia, challenging social behaviors, sexual behaviors, pillaging and hoarding, anxiety/fear, forgetfulness, *Recognize Triggers
Behavior: Agitation Agitation Emotional state of excitement or restlessness. Causes: over stimulation, noise, other resident’s behaviors, pain, hunger, physical need not being met, ect. Signs:pacing, rocking, staring, rigid body posture, cursing, threatening words or gestures, clenched fist Interventions: Remove triggers, keep routine, focus on familiar activity, remain calm, and soothe, but using a firm, non scolding tone of voice, decrease stimulation, touch, do not punish, avoid arguing, redirect by distracting with a familiar task
Behavior-Wandering/Pacing Pacing and Wandering Walking back and forth in the same area or walking aimlessly. Causes:restlessness, hunger, disorientation, need for toileting, constipation, pain, forgetting how or where to sit down, too much napping, need for exercise Interventions: remove causes, give snacks, encourage exercise, maintain toileting schedule, let pace in safe place, and suggest another activity, monitor for fall risk
Behavior: Elopement Elopement Situation where resident left facility without notifying staff Causes: wanting to go “home,” “supposed to be somewhere” Signs: verbalizing wanting to leave, packing belongings, staying near doors, trying to open doors or windows, shaking door handles Interventions: redirect and try to engage the resident in other activities, ensure doors remain secured and alarms are functional, report missing resident immediately
Behavior-Hallucinations/Delusions Hallucination Seeing, hearing, smelling, and feeling something that is not real Delusion Thought or idea not able to be proven by reality Causes: acute illness, or psychiatric condition or cognitive impairment Interventions: ignore if harmless, reassure, do not argue, however do not reinforce false ideas, stay calm, redirect to a reality activity, change the subject if able.
Behavior: Sundowning Sundowning Behavior changes that occur in the evening when darkness arrives, with improvement or resolution during the day. Causes: Unknown Signs: Confusion, restlessness, agitation in the evening hours Interventions: remove triggers, avoid stress, play soft music, set bedtime routine, plan calming activity, remove caffeine, give back massage, distract, and encourage daily exercise. *Facilities to consider the need for more activities or staff during the evening when residents are still awake
Behavior-Catastrophic Reaction Catastrophic Reactions Overreacting and/or unreasonable response to stimuli. Causes: fatigue, over stimulation Signs: exaggerated shouting, hitting, crying, laughing loudly out of context Interventions: Avoid triggers such as fatigue, changes, overstimulation, difficult choices/tasks, pain, hunger, or need for toileting. Remove triggers and distract, offer favorite food or beverage
Behavior: Repetitive Phrasing Perseveration or Repetitive Phrasing Involuntary, uncontrollable repetition of the same word or phrase; often repeating something someone else just said. Causes: habit or hearing a particular phrase, boredom, unmet physical need Intervention: respond with patience, do not stop behavior, and answer questions each time, using the same words, offer food or fluids, engage in calm activity, never mock or encourage behavior.
Behavior: Violence/Aggression Violent Behavior Hitting, biting, kicking screaming, threatening Causes: delusions, hallucinations, acute illness, pain, hunger, excessive noise Signs: pacing, rocking, staring, rigid body posture, clenched fists, getting into someone’s face, threatening words or gestures, slamming doors, or cursing. Interventions: block blows, never hit back, step out of reach, call for help, do not leave resident alone, remove triggers, and use calming techniques.
Behavior: Disruptive Disruptiveness Causing or tending to cause disruption/interference Causes: delusions, hallucinations, acute illness, cognitive impairment, another resident, pain, hunger/thirst, boredom Interventions: Gain resident’s attention, be calm, direct to a private area, ask about behavior, notice and praise improvements, tell resident about changes, encourage to join in activities, help find ways to cope, and focus on positive activities.
Behavior-Paranoia Paranoia Suspicion and mistrust of people or their actions without justification Signs: fearful belief that people are talking about them, stealing their possessions or poisoning their food, withdrawn, refuse to leave their room Causes: Cognitive impairment, mental conditions Interventions: Remain calm and logical, avoid arguing, don’t mock or punish resident, emphasize that staff will always keep them safe.
Challenging Social Behavior Causes: delusions, hallucinations, acute illness, cognitive impairment, or response to interaction with another resident Signs: making mean offensive remarks towards another resident or staff Interventions: Do not take it personally, stay calm, reassure, find out cause, direct to private area, respond positively to appropriate behavior, and report abuse to nurse.
Inappropriate Sexual Behaviors Causes: Provoked by something they heard, saw or thought Signs: Making uncomfortable comments to another resident or staff member Interventions: Be matter-of-fact, be sensitive, distract, direct to private area, and consider other ways to provide physical stimulation, do not over react, remain professional, report incident to nurse
Behavior: Pillaging/Hoarding Pillaging Taking items that belong to another resident or person Hoarding Collecting, hiding, and storing items in a guarded manner Causes: psychiatric diagnosis, cognitive impairment Signs: Residents missing belongings, resident wandering into other resident’s rooms, drawers full of a particular item Interventions: Label belongings, place a label or symbol on door, do not tell others that person is stealing, prepare the family, ask family to report unfamiliar items, and provide a rummage drawer.
Behaviors: Others Anxiety/Fear: Explain procedures, observe body language and be aware of your own body language that could appear threatening to residents Forgetfulness: Do not show annoyance, avoid negative facial expressions, tone of voice, and body language, repeat answers to questions with same words used previously Aphasia: Use gestures, written words, and pictures to help them communicate and avoid frustration, agitation, and unwanted behaviors/challenges
Behavior: Depression Depression Prolonged feelings or profound sadness or hopelessness Causes: loss of independence, inability to cope, feelings of failure and fear, facing incurable illness, chemical imbalance, beginning stages of dementia Signs: loss of appetite or over eating, weight loss or gain, insomnia, sleeping longer than usual, constant exhaustion, varied physical complaints, withdraw/lose interest Interventions: Report signs, encourage independence, talk about moods and feelings, and encourage social interaction.
Methods/Therapies to Reduce Challenging Behaviors • Reality orientation • Useful in early stages of AD • Involves use of calendars, clocks, signs, and lists • May frustrate residents in later stages of AD • Validation therapy • Involves letting residents believe they live in the past or in imaginary circumstances • Can give comfort and reduce agitation • Useful in cases of moderate to severe disorientation
Methods/Therapies to Reduce Challenging Behaviors • Reminiscence therapy • Involves encouraging residents to remember and talk about the past • Should focus on a time of life that was pleasant • Useful in many stages of AD, but especially with moderate to severe confusion • Activity therapy • Uses activies resident enjoys to prevent boredom and frustration • Promotes self-esteem • Useful in most stages of AD
Methods/Therapies to Reduce Challenging Behaviors -Music Therapy: • Sensory stimulation • Hearing familiar songs can be very soothing -Redirection: • change residents focus in a calm, gentle manner • Routine, Routine, Routine
~Define depression. ~List the types of deterioration that occur with dementia. ~List the behaviors that are common with advanced dementia. ~Explain how a CNA should respond to a resident who is exhibiting difficult behaviors. ~Identify techniques that can be used to reduce the effects of dementia. Cognitive ImpairmentLesson 21: Objectives