Download

1 / 30
330 likes | 981 Views
Endoscopic mucosal resection vs radiofrequency ablation in Barrett’s Esophagus. Pietro Dulbecco. UNIVERSITA’ DEGLI STUDI DI GENOVA.

E N D
Endoscopic mucosal resection vs radiofrequency ablation in Barrett’s Esophagus Pietro Dulbecco UNIVERSITA’ DEGLI STUDI DI GENOVA
The overall goal of endoscopic therapy is the complete and durable elimination of esophageal columnar mucosa to ultimately decrease the incidence of esophageal adenocarcinoma, of which BE is the strongest risk factor TechniquesforendoscopiceradicationofBarrett’s Esophagus . Non Tissue-acquiring ablative therapies
TechniquesforendoscopiceradicationofBarrett’s Esophagus • What Is the Role for EMR in Barrett’s Esophagus? • Should Endoscopic Eradication Be Used to Treat Patients Who Have Barrett’s Esophagus With High-Grade Dysplasia or Intramucosal Carcinoma? • ShouldEndoscopicEradication Be Used to Treat Patients Who Have Barrett’s Esophagus With Low-GradeDysplasia? • ShouldEndoscopicEradication Be Used to Treat Patients WhoHaveBarrett’s EsophagusWithoutDysplasia? AGA Technical review-Management of Barrett’s Esophagus. Gastroenterology 2011
TechniquesforendoscopiceradicationofBarrett’s Esophagus • What Is the Role for EMR in Barrett’s Esophagus? • Should Endoscopic Eradication Be Used to Treat Patients Who Have Barrett’s Esophagus With High-Grade Dysplasia or Intramucosal Carcinoma? • ShouldEndoscopicEradication Be Used to Treat Patients Who Have Barrett’s Esophagus With Low-GradeDysplasia? • ShouldEndoscopicEradication Be Used to Treat Patients WhoHaveBarrett’s EsophagusWithoutDysplasia? AGA Technical review-Management of Barrett’s Esophagus. Gastroenterology 2011
TechniquesforendoscopiceradicationofBarrett’s Esophagus EndoscopicmucosalresectionTechnique “en bloc” Piecemeal Namasivayam et al Clinical Gastroenterol and Hepatol 2010; 8:743-754
TechniquesforendoscopiceradicationofBarrett’s Esophagus EndoscopicmucosalresectionTechnique Lift-and-snaretechnique Pouw Re et al Best Prac & ResClinicalGastroenterol 2008;. 22 (5): 929–943
TechniquesforendoscopiceradicationofBarrett’s Esophagus EndoscopicmucosalresectionTechnique Lift-suck-and-cut technique Ligate-and-cuttechnique Pouw Re et al Best Prac & ResClinicalGastroenterol 2008;. 22 (5): 929–943
TechniquesforendoscopiceradicationofBarrett’s Esophagus Why Endoscopic mucosal resection (EMR) is helpful? Depth of invasion of superficial neoplastic lesions arising in Barrett’s esophagus as evaluated in EMR specimens: m1, intraepithelial high-gradedysplasia; m2, intramucosal carcinoma invading the lamina propria; m3, cancer invading into but not through the muscularis mucosae; sm, submucosalinvasion.
TechniquesforendoscopiceradicationofBarrett’s Esophagus Why Endoscopic mucosal resection (EMR) is helpful? Results of histological examination of EMR specimens compared with initial diagnosis in 40 patients with Barrett’s esophagus and HGD or EC 44.8 % (22 of 49) patients had their pathological diagnosis altered by mucosal resection specimen acquisition. EMR upstaged 7 of 49 (14 % ) and downstaged 15 of 49 (31 % ) of patients ’final pathology when compared with pre-EMR biopsy results. Larghi A et al GIE 2005; 62:16-23 Chennat J et al AJG 2009; 104:2684–2692;
TechniquesforendoscopiceradicationofBarrett’s Esophagus • What Is the Role for EMR in Barrett’s Esophagus? • Should Endoscopic Eradication Be Used to Treat Patients Who Have Barrett’s Esophagus With High-Grade Dysplasia or Intramucosal Carcinoma? • ShouldEndoscopicEradication Be Used to Treat Patients Who Have Barrett’s Esophagus With Low-GradeDysplasia? • ShouldEndoscopicEradication Be Used to Treat Patients WhoHaveBarrett’s EsophagusWithoutDysplasia? AGA Technical review-Management of Barrett’s Esophagus. Gastroenterology 2011
TechniquesforendoscopiceradicationofBarrett’s Esophagus Characteristics of EMR studies in Barrett’sb esophagus with HGD/IMCA Focal EMR
TechniquesforendoscopiceradicationofBarrett’s Esophagus Focal EMR: Outcomes Recurrence after 36 and 63 months, respectively Complete response % %
TechniquesforendoscopiceradicationofBarrett’s Esophagus Circumferenzial EMR
TechniquesforendoscopiceradicationofBarrett’s Esophagus Circumferenzial EMR : Outcomes % Pouw 2008 Peters 2006 Larghi 2007 Lopes 2007
TechniquesforendoscopiceradicationofBarrett’s Esophagus Post-EMR complications/limitations % Bleeding : 0.6-11% Perforation : 0.6-11% strictures : 6-37% Bleeding Strictures Perforation Recurrence Prasad GA et al. Gastroenterology 2009;137:815-823 Pech O et . Gut 2008; 57:1200-1206 Chennat J et al. AJG 2009 104:2684-2692
TechniquesforendoscopiceradicationofBarrett’s Esophagus Radiofrequencyablation in Barrett’s Esophagus (HALO System) Frederike G.I. GIE Clin N Am 2010; 20: 55–74
TechniquesforendoscopiceradicationofBarrett’s Esophagus The ablation procedure using the HALO system Frederike G.I. GIE Clin N Am 2010; 20: 55–74
TechniquesforendoscopiceradicationofBarrett’s Esophagus Endoscopic appearance of a focal ablation procedure using the HALO system Frederike G.I. GIE Clin N Am 2010; 20: 55–74
TechniquesforendoscopiceradicationofBarrett’s Esophagus Efficacy of Radiofrequency ablation combined with Endoscopic Resection for Barrett’s Esophagus with HGD and early neoplasia METHODS: 24 patients (mean age, 65 years; median Barrett’s esophagus, 8 cm), with Barrett’s esophagus of ≤12 cm containing HGD or early cancer, from 3 European tertiary-care medical centers Visible lesions were endoscopically resected, followed by serial RFA. Focal escape endoscopic resection was used if Barrett tissue persisted despite RFA Complete response, defined as all biopsies negative for intestinal metaplasia and neoplasia, was assessed during endoscopy with 4-quadrant biopsies taken every 1 cm of the original Barrett’s segment 2 months after the patient was last treated. Pouw RE et al CGH; 2010;8:23–29
TechniquesforendoscopiceradicationofBarrett’s Esophagus Efficacy of Radiofrequency ablation combined with Endoscopic Resection for Barrett’s Esophagus with early neoplasia RESULTS: Twenty-three patients underwent pre-RFA endoscopic resection for visible lesions: 16 IMCA and 7 HGIN. The worst residual histology results, pre-RFA (after any endoscopic resection) were: HGIN (10 patients),LGD (11 patients), and IM (3 patients). Pouw RE eta al CGH; 2010;8:23–29
TechniquesforendoscopiceradicationofBarrett’s Esophagus Efficacy of Radiofrequency ablation combined with Endoscopic Resection for Barrett’s Esophagus with early neoplasia RESULTS: Neoplasia and intestinal metaplasia were eradicated in 95% and 88% of pts, respectively; After escape endoscopic resection in 2 patients, rates improved to 100% and 96%, respectively. After additional follow-up (median, 22 months)no neoplasia recurred Pouw RE eta al CGH; 2010;8:23–29
TechniquesforendoscopiceradicationofBarrett’s Esophagus Conclusions: In patients with BO < 5 cm containing HGD/EC, SRER and ER/RFA achieved comparably high rates of CR-IM and CR-neoplasia. However, SRER was associated with a higher number of complications and therapeutic sessions. For these patients, a combinedendoscopic approach of focal ER followed by RFA may thus be preferred over SRER. Pouw RE etal Gut; 2011;60:765–773
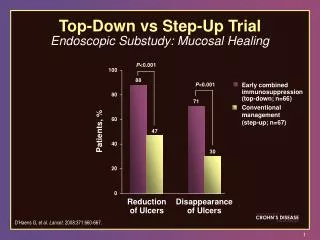
TechniquesforendoscopiceradicationofBarrett’s Esophagus Radiofrequency ablation in Barrett’s Esophagus with HGD P<0.001 control abaltion Percent of Patients with Complete Eradication of Intestinal Metaplasia or Dysplasia at 12 Mo HGD cancer: 1/42 (2%) Complete eradication of intestinal metaplasia (all patients) Complete eradication of HGD Complete eradication of LGD Shaheen NJ et al N Engl J Med 2009;360:2277-88.
TechniquesforendoscopiceradicationofBarrett’s Esophagus • What Is the Role for EMR in Barrett’s Esophagus? • ShouldEndoscopic Eradication Be Used toTreat Patients Who Have Barrett’s EsophagusWithHigh-GradeDysplasia or Intramucosal Carcinoma? • Should Endoscopic Eradication Be Used to Treat Patients Who Have Barrett’s Esophagus With Low-Grade Dysplasia? • ShouldEndoscopicEradication Be Used to Treat Patients WhoHaveBarrett’s EsophagusWithoutDysplasia? AGA Technical review-Management of Barrett’s Esophagus. Gastroenterology 2011
TechniquesforendoscopiceradicationofBarrett’s Esophagus Radiofrequency ablation in Barrett’s Esophagus with LGD P<0.001 control abaltion Percent of Patients with Complete Eradication of Intestinal Metaplasia or Dysplasia at 12 Mo LGD HGD: 2/42 (5%) Complete eradication of HGD Complete eradication of intestinal metaplasia (all patients) Complete eradication of LGD Shaheen NJ et al N Engl J Med 2009;360:2277-88.
TechniquesforendoscopiceradicationofBarrett’s Esophagus Durability of RFA in Barrett’s esophagus with dysplasia More than 85% of HGD patients and 90% of LGD patients remained free of dysplasia at a mean follow-up of longer than 3 years with no additional therapy. More than 75% of HGD patients and LGD patients remained free of IM, again with follow-up of longer than 3 years, with no additional therapy. Shaheen NJ et al Gastroenterology 2011;141:460-468.
Endoscopic radiofrequency ablation of Barrett’s esophagus without dysplasia Circumferential ablation of nondysplastic BE by using this balloon-based ablation device can be performed with no subsequent strictures or buried glands and with complete elimination of BE in 70% of patients at 1-year follow-up. TechniquesforendoscopiceradicationofBarrett’s Esophagus RESULTS: In the effectiveness phase, 70 patients (52 men, 18 women; mean age, 55.7 years) were enrolled. At 12 months CR for BE was achieved in 70% of patients. There were no strictures and no buried glandular mucosa in either study phase (4306 biopsy fragments evaluated). Conclusions: Sharma VK et al Gastrointest Endosc 2007;65:185-95
Endoscopic radiofrequency ablation of Barrett’s esophagus without dysplasia TechniquesforendoscopiceradicationofBarrett’s Esophagus Circumferential ablation was performed at baseline and repeated at 4 months if there was residual IM. Follow-up biopsy specimens were obtained at 1, 3, 6, 12, and 30 months.. Focal ablation was performed after the 12-month follow-up for histological evidence of IM at the 12-month biopsy (absolute indication) or endoscopic appearance suggestive of columnar-lined esophagus (relative indication). RESULTS: At 12 months, CR-IM was achieved in 48 of 69 available patients (69%) At 30 months after additional focal ablative therapy, CR-IM was achieved in 60 of 61 available patients (97%). There were no strictures or buried glandular mucosa detected by the standardized biopsy protocol at 12 or 30 months, and there were no serious adverse events. Fleisher DE et al Gastrointest Endosc 2008;68:867-76
TechniquesforendoscopiceradicationofBarrett’s Esophagus Conclusions: What is the optimal role of endoscopic mucosal resection? • EMR can be considered a valuable diagnostic/ staging procedure for identifying submucosal invasion that might not be apparent by less invasive techniques such as mucosal biopsy and EUS. • The key unresolved issue is the role of circumferential endoscopic mucosal resection. • What is the optimal technique? • 2. Should it be limited to patients with nodules only, or should it be applied in patients with flat dysplasia? • 3. What is the optimal role and setting for circumferential endoscopic mucosal resection? • 4. Can complications, especially strictures, be avoided?
TechniquesforendoscopiceradicationofBarrett’s Esophagus Conclusions: What is the optimal role of RF • RFA is effective, safe, and well tolerated in the treatment ofnondysplasticand dysplastic BE • RFA provides safe and cost-effective alternative to surgery or surveillance in the management of HGD • Its role in the setting of LGD and non dysplastic disease is less clear, but there is evidence of durable reversion and cost-effectiveness in this group • Further studies should be performed to determine the durability of RFA and the appropriate surveillance protocl following ablation