Download
1 / 26
260 likes | 414 Views
Salman Bin AbdulAziz University College Of Pharmacy. PAH. Mohammad Ruhal Ain R Ph, PGDPRA, M Pharm ( Clin . Pharm ) Department of Clinical Pharmacy. Case 1.

E N D
Salman Bin AbdulAzizUniversity College Of Pharmacy PAH Mohammad RuhalAin R Ph, PGDPRA, M Pharm (Clin. Pharm) Department of Clinical Pharmacy
Case 1 R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of breath. She could walk only 10–20 ft at baseline and is now short of breath at rest. Her arterial blood gas is pH 7.31/Pco2 65/Po2 53/85% O2 saturation. She has three-pillow orthopnea and 3+ pitting edema in her lower extremities. Medical history significant only for AF. Computerized tomographic angiography shows that her pulmonary artery trunk is substantially enlarged, with a mean pressure of 56 mm Hg. On Examnination Echocardiography shows right atrial and ventricular hypertrophy. Chest radiography detects prominent interstitial markings.
laboratory test BUN 21 mg/dL, SCr 1.2 mg/dL, AST 145 IU/L, ALT 90 IU/L, INR 2.1, and PTT 52 seconds; vital signs include BP 108/62 mm Hg and HR 62 beats/minute. Home medications warfarin 2.5 mg/day, ipratropium 2 puffs every 6 hours, salmeterol 2 puffs 2 times/day, and diltiazem 480 mg/day. Her diagnosis is IPAH. Define ! •PAH (Pulmonary Arterial Hypertension) •Types of PAH ? •Complications of PAH include ? 1. right ventricular dysfunction leading to right heart failure. 2. Blood clots 3. Irregular heartbeats (arrhythmias)
The ( S , O ) ( signs and symptoms ) part of SOAP in this patient is ? • Subjective • increasing symptoms of fatigue and shortness of breath. She could walk only 10–20 ft at baseline and is now short of breath at rest • Objective • arterial blood gas is pH 7.31/Pco2 65/Po2 53/85% O2 saturation. She has three-pillow orthopnea and 3+ pitting edema in her lower • Medical history • significant only for AF. Computerized tomographic angiography shows that her pulmonary artery trunk is substantially enlarged, with a mean pressure of 56 mm Hg • On Examnination • Echocardiography shows right atrial and ventricular hypertrophy. Chest radiography detects prominent interstitial markings. • Medications • warfarin 2.5 mg/day, ipratropium 2 puffs every 6 hours, salmeterol 2 puffs 2 times/day, and diltiazem 480 mg/day.
MCQ •All the following procedures used to diagnose R.W condition except I.Electrocardiogram (ECG ), Echocardiography ,hemodynamic changes II.Chest radiography III.Physical examination IV.Spirometry
MCQ •All the following procedures used to diagnose R.W condition except I.Electrocardiogram (ECG ), Echocardiography ,hemodynamic changes II.Chest radiography III.Physical examination IV.Spirometry Complete Patients with PAH, Chest radiography shows ? Enlarged pulmonary arteries and diminished peripheral pulmonary vascular Patient with PAH , physical examination shows ?
R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of breath. She could walk only 10–20 ft at baseline and is now short of breath at rest. Her arterial blood gas is pH 7.31/Pco2 65/Po2 53/85% O2 saturation. She has three-pillow orthopnea and 3+ pitting edema in her lower extremities. Question: According to WHO classification ,this patient has I.Class I PAH II.Class II PAH III.Class III PAH IV.Class IV PAH
Functional class I–II, ambulated 380 m or greater (or 1250 ft) during 6-minute walk test,
R.W. is a 38-year-old obese woman who presents with increasing symptoms of fatigue and shortness of breath. She could walk only 10–20 ft at baseline and is now short of breath at rest. Her arterial blood gas is pH 7.31/Pco2 65/Po2 53/85% O2 saturation. She has three-pillow orthopnea and 3+ pitting edema in her lower extremities. Question: According to WHO classification ,this patient has I.Class I PAH II.Class II PAH III.Class III PAH IV.Class IV PAH
•In PAH patient like R.W , goals of therapy include the following except ? I.Curing PAH II.Relieve acute dyspnea symptoms. III.Improve exercise capacity/quality of life and prevent death.
•In PAH patient like R.W , goals of therapy include the following except ? I.Curing PAH II.Relieve acute dyspnea symptoms. III.Improve exercise capacity/quality of life and prevent death. Goals of therapy I.Relieve acute dyspnea symptoms. II.Improve exercise capacity/quality of life and prevent death.
Question: •How to assess the response to the treatment of mr R.W. Condition A.functional class determination ( WHO classification for PAH) B.6 min walk test (every 4–6 Months) C.ChestXray D.A and B E.All of the above
Question: •How to assess the response to the treatment of mr R.W. Condition A.functional class determination ( WHO classification for PAH) B.6 min walk test (every 4–6 Months) C.ChestXray D.A and B E.All of the above
What are the Satisfactory condition in a patient with PAH ? I. Functional class I–II, II. ambulated 380 m or greater or 1250 ft) during 6-minute walk test, III. CI of 2.2 L/minute/m2 or greater IV. and mPAP less than 12 mm Hg
What are the Satisfactory condition in a patient with PAH ? I. Functional class I–II, II. ambulated 380 m or greater or 1250 ft) during 6-minute walk test, III. CI of 2.2 L/minute/m2 or greater IV. and mPAP less than 12 mm Hg
Case Remaining part increasing symptoms of fatigue and shortness of breath. She could walk only 10–20 ft at baseline and is now short of breath at rest. Her arterial blood gas is pH 7.31/Pco2 65/Po2 53/85% O2 saturation. She has three-pillow orthopnea and 3+ pitting edema in her lower extremities. laboratory test BUN 21 mg/dL, SCr 1.2 mg/dL, AST 145 IU/L, ALT 90 IU/L, INR 2.1, and PTT 52 seconds; vital signs include BP 108/62 mm Hg and HR 62 beats/minute. Home medications warfarin 2.5 mg/day, ipratropium 2 puffs every 6 hours, salmeterol 2 puffs 2 times/day, and diltiazem 480 mg/day. Her diagnosis is IPAH.
Question: Based on the options below, which one of the following is the best evidence-based management strategy? A. Increase diltiazem to 600 mg/day. B. Start sildenafil 20 mg 3 times/day. C. Start epoprostenol 2 ng/kg/minute. D. Start bosentan 62.5 mg 2 times/day.
Question: Based on the options below, which one of the following is the best evidence-based management strategy? A. Increase diltiazem to 600 mg/day. B. Start sildenafil 20 mg 3 times/day. C. Start epoprostenol 2 ng/kg/minute. D. Start bosentan 62.5 mg 2 times/day. - She is taking a considerable dose of diltiazem, and her HR likely will not tolerate further increases in therapy. - bosentanis an attractive oral option to manage her PAH, her liver enzymes are elevated more than 3 times the upper limit of normal - Because this patient is currently in functional class IV with symptoms at rest, epoprostenol is indicated for a survival benefit.
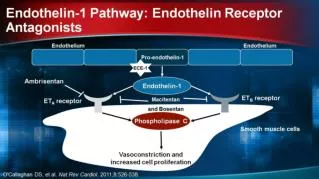
•Adverse effects of epoprostenol ? •Adverse effects of CCB ? •When treating a patient with PAH , we select CCB agent on the basis of HR at baseline If tachycardic, choose …………………. If bradycardic, choose ………….. , ………….. True or false CCB in PAH should be used empirically without postive response to acute vasodilatory response testing! •Bosentan belongs to which class ? •What monitoring parameters should be taken care of when starting patient on bosentan •Sildenafil and Tadalafil adverse effects and mention a difference between the two drugs