Download
1 / 15
150 likes | 154 Views
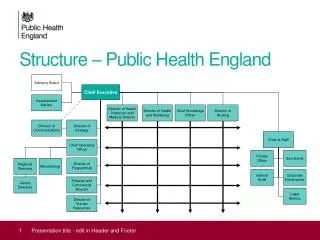
Medications in recovery: re-orientating drug dependence treatment How can we make Shared-care in Wandsworth more recovery orientated?. Hannah Lindsell Public Health England. In a nutshell…. The group’s final report A lot done. A lot more to do!. Key principles.

E N D
Medications in recovery: re-orientating drug dependence treatmentHow can we make Shared-care in Wandsworth more recovery orientated? Hannah Lindsell Public Health England
In a nutshell… The group’s final report A lot done. A lot more to do!
Key principles Everyone can recover, but not everyone will We don’t know who will Give everyone the best chance for long term recovery Make leaving treatment and sustained recovery a hope for all from the beginning
Drug treatment has been a big success story • Lives saved, harms reduced • HIV rates amongst IV drug users are down • Injecting rates amongst drug users are down • Drug related deaths are down • Crime has been much reduced
The problem • 2010 drug strategy: • “Substitute prescribing continues to have a role to play in the treatment of heroin dependence, both in stabilising drug use and supporting detoxification. Medically-assisted recovery can, and does, happen… • However, for too many people currently on a substitute prescription, what should be the first step on the journey to recovery risks ending there. This must change.”
The group’s final report – July 2012 • High-quality treatment system that substantially improves health • Heroin is sticky • Leaving treatment is important but it isn’t recovery • Lots of people haven’t recovered • Done right, OST is effective but a platform for recovery • Don’t end it too early • Some people recover fast, some don’t – all need recovery support
Avoid unintended consequences • Let’s be clear: • This is about increasing recovery-oriented ambition and progress for individuals and in systems where there is not currently enough of it • It is not about destabilising - to the point of unacceptable risk - individuals who are deriving benefit from OST.
Key to success • A shared vision of recovery, and leadership • Organisations & staff able to support and sustain change • Staff who believe in the treatment they are delivering • A structured programme with clear treatment goals • Availability and range of OST medications • Range and quality of psychosocial interventions • Active referral to self help and mutual aid • Links to recovery orientated community organisations
The evidence ... • ... is good that OST: • Retains people in treatment • Suppresses illicit use of heroin • Reduces crime • Reduces the risk of BBV • Reduces risk of death. • ... is less persuasive that OST: • Suppresses other drug use • Improves physical and mental health • Improves social reintegration of marginalised heroin users • Promotes abstinence from all drugs.
What should services do? • Do more, and review more frequently • Do it quickly for those new in treatment, and purposefully for all • Review those in long term treatment to check that they are still benefitting. If not, adjust treatment • But avoid unintended consequences (exiting too soon and returning)
What shared care looks like in Wandsworth • Nurse practitioner model • GP Prescribing/Pharmacological interventions-325 • 48/325 = Non-Opiate • 277/325 = Opiate • Total number in treatment = 860 • 325/860 = 38% (LONDON average = 37%) • Percentage of GP prescribing patients that successfully complete = 6% (LONDON average = 5%) • Length of GP prescribing/Pharmacological intervention: • 0-1yrs-76% • 2-5 yrs- 24% • 6+ years-0%
Recovery support-what does it look like in Wandsworth? • Peer-role models and peer support • Employment support • Family and social networks • Housing support • Mutual Aid-NA, CA, AA, Smart Recovery?
What are the challenges for Wandsworth Shared care? • 15/42 practices engaged-expand? How? What are the barriers? • Opportunity to review model/outcomes every year when you review the LES? • How recovery orientated does the shared care system feel? • Care Plan Audit of Shared Care clients? • How often are Care Plan Review carried out with the Nurse practitioner, the client, the Pharmacist, the GP?
Further challenges? • Low dose for 2-5yrs? Abstinence a realistic option? Is it offered? • Greenwich model-brought in a Psychologist to work with this client group • Is there an opportunity to segment the shared care population?
Any questions? • ? • Hannah.lindsell@phe.gov.uk • 07795 036 473