Download

1 / 34
340 likes | 516 Views
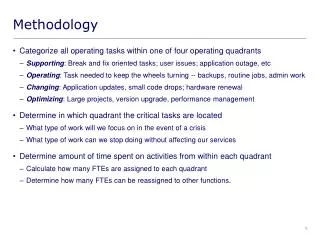
Improvement methodology. “quality improvement”. The combined and unceasing efforts of everyone – health care professionals, patients and their families, researchers, payers, planners, administrators, educators – to make changes that will lead to

E N D
“quality improvement” The combined and unceasing efforts of everyone – health care professionals, patients and their families, researchers, payers, planners, administrators, educators – to make changes that will lead to better patient outcome, better system performance, and better professional development. Batalden P, Davidoff F. Qual. Saf. Health Care 2007;16;2-3
Eras of quality 1) The 1990s – Evidence based medicine LOX-GNH145-20071113-BVJM
Evidence – SIGN 1++ High quality meta-analyses, systematic reviews of RCTs or RCTs with a very low risk of bias 1+ Well conducted meta-analyses, systematic reviews of RCTs or RCTs with a low risk of bias 1- Meta-analyses, systematic reviews or RCTs with a high risk of bias 2++ High quality systematic reviews of case control or cohort studies 2+ Well conducted case control or cohort studies 2- Case control or cohort studies with a high risk of confounding 3 Non-analytic studies – case reports, case series 4 Expert opinion
17 years to apply 14% of research knowledge to patient care! Balas EA, Boren SA. Managing clinical knowledge for health care improvement. Yrbk of Med Informatics 2000; 65-70
Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trialsGordon C S Smith, Jill P Pell. BMJ 2003;327;1459-1461 Aim: To determine whether parachutes are effective in preventing major trauma related to gravitational challenge. Design: Systematic review of randomised controlled trials Results: Our search strategy did not find any randomised controlled trials of the parachute.
Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trialsGordon C S Smith, Jill P Pell. BMJ 2003;327;1459-1461 Conclusion: As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomised controlled trials. Advocates of evidence based medicine have criticised the adoption of interventions evaluated by using only observational data. We think that everyone might benefit if the most radical protagonists of evidence based medicine organised and participated in a double blind, randomised, placebo controlled, crossover trial of the parachute
Eras of quality 2) The 2000s – ADD Evidence based delivery LOX-GNH145-20071113-BVJM
“Society’s huge investment in technological innovations that only modestly improve efficacy, by consuming resources needed for improved delivery of care, may cost more lives than it saves.” “Health, economic, and moral arguments make the case for spending less on technological advances and more on improving systems for delivering care.”
Fidelity vs Efficacy $100 Million $29 Billion $32 Billion 0.002%
The aspirin example In patients who have had a stroke or TIA aspirin reduces risk by 23% 100,000 patients – 23,000 fewer strokes 58% of eligible patients receive aspirin = 13,340 fewer strokes
Two options Fidelity – increase to 100% of eligible patients = 9,660 strokes Efficacy – requires a proportional improvement over aspirin of 74% Clopidogrel = 10% more efficacy than aspirin
The “Quality Curve” Shift and narrow the curve: What is the norm? 2 3 1 Cut the tail: What is unacceptable? Extend the ambition: What is great? (What is possible?)
What is a Bundle? It is a set of evidence based steps that experts believe are critical Having the steps joined provides a “forcing function.” Evidence based medicine Evidence based care delivery
Bundle Implementation The steps must all be completed to succeed The “all or none” feature is the source of the bundle’s power Pass/fail
Ventilator Bundle Elevating the head of the patient’s bed Daily "sedation vacations," or gradually lightening the use of sedatives each day Daily assessment of the patient’s readiness to extubate or wean from the ventilator Chlorhexidine oral care
103 ICUs Working on Central Line Infections: • 82% Reduction in Mean Rate • 1,578 Lives Saved • 81,020 Hospital Days Saved • “Over $165million in costs averted” 30
Proposed New Quality Aims To make NHS Scotland a world leader in healthcare quality improvement. To do so in a way that is meaningful to all.
“Expectations will always exceed capacity. The service must always be changing, growing and improving…”. Aneurin Bevan, 1948