Download
1 / 1
30 likes | 229 Views
MEMBRANOPROLIFERATIVE GLOMERULONEPHRITIS IN THE SETTING OF MULTICENTRIC ANGIOFOLLICULAR LYMPH NODE HYPERPLASIA (CASTLEMAN’S DISEASE) COMPLICATED BY EVAN’S SYNDROME Gakiopoulou H, Paraskevakou H, Marinaki S, Voulgarelis M, Korkolopoulou P, Lazaris A, Tzirakis M, Stofas A,

E N D
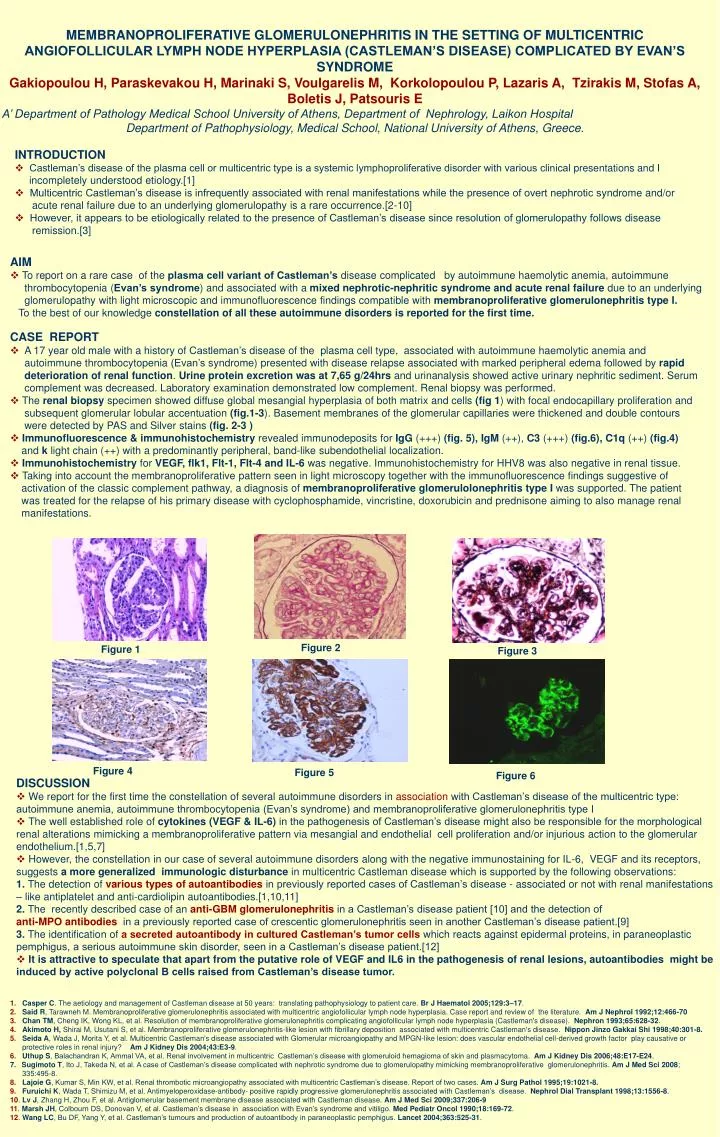
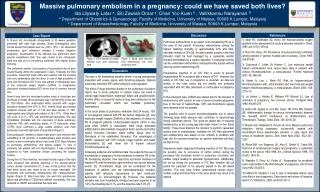
MEMBRANOPROLIFERATIVE GLOMERULONEPHRITIS IN THE SETTING OF MULTICENTRIC ANGIOFOLLICULAR LYMPH NODE HYPERPLASIA (CASTLEMAN’S DISEASE) COMPLICATED BY EVAN’S SYNDROME Gakiopoulou H, Paraskevakou H, Marinaki S, Voulgarelis M, Korkolopoulou P, Lazaris A, Tzirakis M, Stofas A, Boletis J, Patsouris E A’ Department of Pathology Medical School University of Athens, Department of Nephrology, Laikon Hospital Department of Pathophysiology, Medical School, National University of Athens, Greece. • INTRODUCTION • Castleman’s disease of the plasma cell or multicentric type is a systemic lymphoproliferative disorder with various clinical presentations and I incompletely understood etiology.[1] • Multicentric Castleman’s disease is infrequently associated with renal manifestations while the presence of overt nephrotic syndrome and/or acute renal failure due to an underlying glomerulopathy is a rare occurrence.[2-10] • However, it appears to be etiologically related to the presence of Castleman’s disease since resolution of glomerulopathy follows disease remission.[3] • AIM • To report on a rare case of the plasma cell variant of Castleman’s disease complicated by autoimmune haemolytic anemia, autoimmune thrombocytopenia (Evan’s syndrome) and associated with a mixed nephrotic-nephritic syndrome and acute renal failure due to an underlying glomerulopathy with light microscopic and immunofluorescence findings compatible with membranoproliferative glomerulonephritis type I. • To the best of our knowledge constellation of all these autoimmune disorders is reported for the first time. • CASE REPORT • A 17 year old male with a history of Castleman’s disease of the plasma cell type, associated with autoimmune haemolytic anemia and autoimmune thrombocytopenia (Evan’s syndrome) presented with disease relapse associated with marked peripheral edema followed by rapid deterioration of renal function. Urine protein excretion was at 7,65 g/24hrs and urinanalysis showed active urinary nephritic sediment. Serum complement was decreased. Laboratory examination demonstrated low complement. Renal biopsy was performed. • The renal biopsy specimen showed diffuse global mesangial hyperplasia of both matrix and cells (fig 1) with focal endocapillary proliferation and subsequent glomerular lobular accentuation (fig.1-3). Basement membranes of the glomerular capillaries were thickened and double contours were detected by PAS and Silver stains (fig. 2-3 ) • Immunofluorescence & immunohistochemistry revealed immunodeposits for IgG (+++) (fig. 5),IgM (++), C3 (+++) (fig.6),C1q (++) (fig.4) and k light chain (++) with a predominantly peripheral, band-like subendothelial localization. • Immunohistochemistry for VEGF, flk1, Flt-1, Flt-4 and IL-6 was negative. Immunohistochemistry for HHV8 was also negative in renal tissue. • Taking into account the membranoproliferative pattern seen in light microscopy together with the immunofluorescence findings suggestive of activation of the classic complement pathway, a diagnosis of membranoproliferative glomerulolonephritis type I was supported. The patient was treated for the relapse of his primary disease with cyclophosphamide, vincristine, doxorubicin and prednisone aiming to also manage renal manifestations. Figure 2 Figure 1 Figure 3 Figure 4 Figure 5 Figure 6 • DISCUSSION • We report for the first time the constellation of several autoimmune disorders in association with Castleman’s disease of the multicentric type: autoimmune anemia, autoimmune thrombocytopenia (Evan’s syndrome) and membranoproliferative glomerulonephritis type I • The well established role of cytokines (VEGF & IL-6) in the pathogenesis of Castleman’s disease might also be responsible for the morphological renal alterations mimicking a membranoproliferative pattern via mesangial and endothelial cell proliferation and/or injurious action to the glomerular endothelium.[1,5,7] • However, the constellation in our case of several autoimmune disorders along with the negative immunostaining for IL-6, VEGF and its receptors, suggests a more generalized immunologic disturbance in multicentric Castleman disease which is supported by the following observations: • 1. The detection of various types of autoantibodies in previously reported cases of Castleman’s disease - associated or not with renal manifestations – like antiplatelet and anti-cardiolipin autoantibodies.[1,10,11] • 2. The recently described case of an anti-GBM glomerulonephritis in a Castleman’s disease patient [10] and the detection of • anti-MPO antibodies in a previously reported case of crescentic glomerulonephritis seen in another Castleman’s disease patient.[9] • 3. The identification of a secreted autoantibody in cultured Castleman’s tumor cells which reacts against epidermal proteins, in paraneoplastic pemphigus, a serious autoimmune skin disorder, seen in a Castleman’s disease patient.[12] • It is attractive to speculate that apart from the putative role of VEGF and IL6 in the pathogenesis of renal lesions, autoantibodies might be induced by active polyclonal B cells raised from Castleman’s disease tumor. • 1.Casper C. The aetiology and management of Castleman disease at 50 years: translating pathophysiology to patient care. Br J Haematol 2005;129:3–17. • 2.Said R, Tarawneh M. Membranoproliferative glomerulonephritis associated with multicentric angiofollicular lymph node hyperplasia. Case report and review of the literature. Am J Nephrol 1992;12:466-70 • 3.Chan TM, Cheng IK, Wong KL, et al. Resolution of membranoproliferative glomerulonephritis complicating angiofollicular lymph node hyperplasia (Castleman's disease). Nephron 1993;65:628-32. • 4.Akimoto H, Shirai M, Usutani S, et al. Membranoproliferative glomerulonephritis-like lesion with fibrillary deposition associated with multicentric Castleman's disease. Nippon Jinzo Gakkai Shi 1998;40:301-8. • 5.Seida A, Wada J, Morita Y, et al. Multicentric Castleman's disease associated with Glomerular microangiopathy and MPGN-like lesion: does vascular endothelial cell-derived growth factor play causative or • protective roles in renal injury? Am J Kidney Dis 2004;43:E3-9. • 6.Uthup S, Balachandran K, Ammal VA, et al. Renal involvement in multicentric Castleman’s disease with glomeruloid hemagioma of skin and plasmacytoma. Am J Kidney Dis 2006;48:E17-E24. • Sugimoto T, Ito J, Takeda N, et al. A case of Castleman’s disease complicated with nephrotic syndrome due to glomerulopathy mimicking membranoproliferative glomerulonephritis. Am J Med Sci 2008; • 335:495-8. • 8.Lajoie G, Kumar S, Min KW, et al. Renal thrombotic microangiopathy associated with multicentric Castleman’s disease. Report of two cases. Am J Surg Pathol 1995;19:1021-8. • 9.Furuichi K, Wada T, Shimizu M, et al. Antimyeloperoxidase-antibody- positive rapidly progressive glomerulonephritis associated with Castleman’s disease. Nephrol Dial Transplant 1998;13:1556-8. • 10. Lv J, Zhang H, Zhou F, et al. Antiglomerular basement membrane disease associated with Castleman disease. Am J Med Sci 2009;337:206-9 • 11. Marsh JH, Colbourn DS, Donovan V, et al. Castleman’s disease in association with Evan’s syndrome and vitiligo. Med Pediatr Oncol 1990;18:169-72. • 12. Wang LC, Bu DF, Yang Y, et al. Castleman’s tumours and production of autoantibody in paraneoplastic pemphigus. Lancet 2004;363:525-31.
















![Case Report # []](https://cdn3.slideserve.com/6989602/slide1-dt.jpg)