Download
1 / 1

E N D
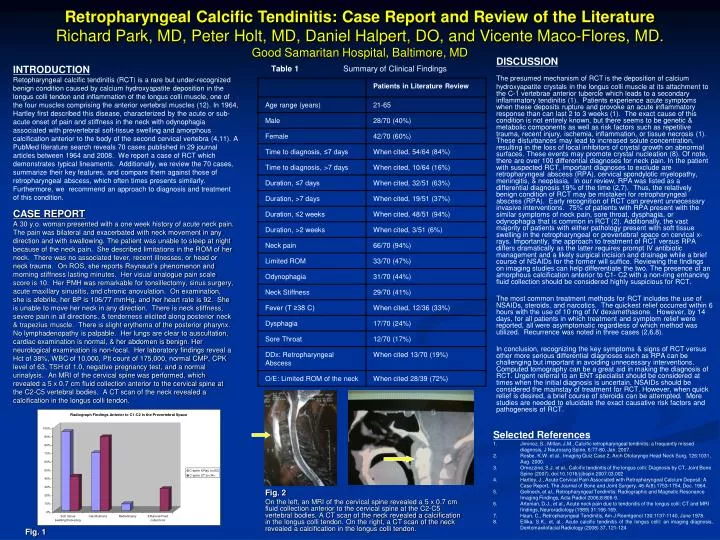
DISCUSSION The presumed mechanism of RCT is the deposition of calcium hydroxyapatite crystals in the longus colli muscle at its attachment to the C-1 vertebrae anterior tubercle which leads to a secondary inflammatory tendinitis (1). Patients experience acute symptoms when these deposits rupture and provoke an acute inflammatory response than can last 2 to 3 weeks (1). The exact cause of this condition is not entirely known, but there seems to be genetic & metabolic components as well as risk factors such as repetitive trauma, recent injury, ischemia, inflammation, or tissue necrosis (1). These disturbances may lead to increased solute concentration, resulting in the loss of local inhibitors of crystal growth on abnormal surfaces. These events may promote crystal nucleation (8). Of note, there are over 100 differential diagnoses for neck pain. In the patient with suspected RCT, important diagnoses to exclude are retropharyngeal abscess (RPA), cervical spondylotic myelopathy, meningitis, & neoplasia. In our review, RPA was listed as a differential diagnosis 19% of the time (2,7). Thus, the relatively benign condition of RCT may be mistaken for retropharyngeal abscess (RPA). Early recognition of RCT can prevent unnecessary invasive interventions. 75% of patients with RPA present with the similar symptoms of neck pain, sore throat, dysphagia, or odynophagia that is common in RCT (2). Additionally, the vast majority of patients with either pathology present with soft tissue swelling in the retropharyngeal or prevertebral space on cervical x-rays. Importantly, the approach to treatment of RCT versus RPA differs dramatically as the latter requires prompt IV antibiotic management and a likely surgical incision and drainage while a brief course of NSAIDs for the former will suffice. Reviewing the findings on imaging studies can help differentiate the two. The presence of an amorphous calcification anterior to C1- C2 with a non-ring enhancing fluid collection should be considered highly suspicious for RCT. The most common treatment methods for RCT includes the use of NSAIDs, steroids, and narcotics. The quickest relief occurred within 6 hours with the use of 10 mg of IV dexamethasone. However, by 14 days, for all patients in which treatment and symptom relief were reported, all were asymptomatic regardless of which method was utilized. Recurrence was noted in three cases (2,6,8). In conclusion, recognizing the key symptoms & signs of RCT versus other more serious differential diagnoses such as RPA can be challenging but important in avoiding unnecessary interventions. Computed tomography can be a great aid in making the diagnosis of RCT. Urgent referral to an ENT specialist should be considered at times when the initial diagnosis is uncertain. NSAIDs should be considered the mainstay of treatment for RCT. However, when quick relief is desired, a brief course of steroids can be attempted. More studies are needed to elucidate the exact causative risk factors and pathogenesis of RCT. Retropharyngeal Calcific Tendinitis: Case Report and Review of the LiteratureRichard Park, MD, Peter Holt, MD, Daniel Halpert, DO, and Vicente Maco-Flores, MD.Good Samaritan Hospital, Baltimore, MD INTRODUCTION Retopharyngeal calcific tendinitis (RCT) is a rare but under-recognized benign condition caused by calcium hydroxyapatite deposition in the longus colli tendon and inflammation of the longus colli muscle, one of the four muscles comprising the anterior vertebral muscles (12). In 1964, Hartley first described this disease, characterized by the acute or sub-acute onset of pain and stiffness in the neck with odynophagia associated with prevertebral soft-tissue swelling and amorphous calcification anterior to the body of the second cervical vertebra (4,11). A PubMed literature search reveals 70 cases published in 29 journal articles between 1964 and 2008. We report a case of RCT which demonstrates typical lineaments. Additionally, we review the 70 cases, summarize their key features, and compare them against those of retropharyngeal abscess, which often times presents similarly. Furthermore, we recommend an approach to diagnosis and treatment of this condition. Table 1 Summary of Clinical Findings CASE REPORT A 30 y.o. woman presented with a one week history of acute neck pain. The pain was bilateral and exacerbated with neck movement in any direction and with swallowing. The patient was unable to sleep at night because of the neck pain. She described limitations in the ROM of her neck. There was no associated fever, recent illnesses, or head or neck trauma. On ROS, she reports Raynaud’s phenomenon and morning stiffness lasting minutes. Her visual analogue pain scale score is 10. Her PMH was remarkable for tonsillectomy, sinus surgery, acute maxillary sinusitis, and chronic anovulation. On examination, she is afebrile, her BP is 106/77 mmHg, and her heart rate is 92. She is unable to move her neck in any direction. There is neck stiffness, severe pain in all directions, & tenderness elicited along posterior neck & trapezius muscle. There is slight erythema of the posterior pharynx. No lymphadenopathy is palpable. Her lungs are clear to auscultation, cardiac examination is normal, & her abdomen is benign. Her neurological examination is non-focal. Her laboratory findings reveal a Hct of 38%, WBC of 10,000, Plt count of 175,000, normal CMP, CPK level of 63, TSH of 1.0, negative pregnancy test, and a normal urinalysis. An MRI of the cervical spine was performed, which revealed a 5 x 0.7 cm fluid collection anterior to the cervical spine at the C2-C5 vertebral bodies. A CT scan of the neck revealed a calcification in the longus colli tendon. • Selected References • Jiminez, S., Millan, J.M., Calcific retropharyngeal tendinitis: a frequently missed diagnosis, J Neurosurg Spine, 6:77-80, Jan. 2007. • Rosbe, K.W. et al., Imaging Quiz Case 2, Arch Otolaryngo Head Neck Surg, 126:1031, Aug. 2000. • Omezzine, S.J. et al., Calcific tendinitis of the longus colli: Diagnosis by CT, Joint Bone Spine (2007), doi:10.1016/j/jbspin.2007.03.002 • Hartley, J., Acute Cervical Pain Associated with Retropharyngeal Calcium Deposit: A Case Report, The Journal of Bone and Joint Surgery, 46-A(8):1753-1754, Dec. 1964. • Gelineck, et al., Retropharyngeal Tendinitis: Radiographic and Magnetic Resonance Imaging Findings, Acta Radiol 2006;8:806-9. • Artenian, D.J., et al., Acute neck pain due to tendonitis of the longus colli: CT and MRI findings, Neuroradiology (1989) 31:166-169. • Haun, C., Retropharyngeal Tendinitis, Am J Roentgenol 130:1137-1140, June 1978. • Ellika, S.K., et. al., Acute calcific tendinitis of the longus colli: an imaging diagnosis, Dentomaxilofacial Radiology (2008) 37, 121-124 • . Fig. 2 On the left, an MRI of the cervical spine revealed a 5 x 0.7 cm fluid collection anterior to the cervical spine at the C2-C5 vertebral bodies. A CT scan of the neck revealed a calcification in the longus colli tendon. On the right, a CT scan of the neck revealed a calcification in the longus colli tendon. Fig. 1